CCA (general clinical analysis) of blood is a clinical and hematological method for assessing the composition of the main biofluid of the body, the purpose of which is to identify possible disorders. The study of blood composition in laboratory conditions is carried out under a microscope (microscopy “manually”) and on hematological automatic analyzers.
The computer records the final data of the automatic calculation and sends it to print. The study form indicates the decoding of the general blood test in Latin letters (an abbreviation for the full name of the indicator).
Manual counting microscopy takes longer but is considered more accurate. The optimally informative assessment option is an automatic analysis, supplemented by the calculation of a leukogram by a laboratory specialist.
Why is this test prescribed?
Urine is a biological fluid in which the final waste products of the body are released from the human body.
It is conventionally divided into primary (formed by filtration in the glomeruli from blood plasma) and secondary (formed by reabsorption of water, necessary metabolites and other solutes in the renal tubules).
Disruption of this system entails characteristic changes in normal TAM indicators. Thus, the analysis can show:
- 1 Metabolic abnormalities;
- 2 Signs of urinary tract infection;
- 3Effectiveness of treatment and diet;
- 4Dynamics of recovery.
A person can contact a laboratory for a urine test on his own initiative if he notices sudden changes in his physical characteristics. But more often the patient receives a referral from a specialist at the clinic, who then deciphers the results obtained.
OAM is included in the list of basic studies during preventive examinations of the population, clinical examination, it is prescribed when seeking medical help from a specialist, during pregnancy, during hospitalization and in some other cases.
A general urine test consists of a sequential study of:
- 1Physical characteristics of the sample;
- 2Chemical composition;
- 3Microscopic examination of sediment.
Indications for use
Clinical urine examination is one of the most widely used tests and is prescribed in the following cases:
- preventive examination during the annual medical examination;
- suspicion of diseases of the urinary system;
- for diagnosing inflammatory processes of internal organs;
- assessment of the dynamics of treatment of the kidneys, bladder and urinary tract, streptococcal infections.
The results of urine parameters are assessed in conjunction with other laboratory tests (complete blood count, stool, etc.).
Patient preparation
Before submitting the material for general (clinical) analysis, consult your doctor about the possible temporary cessation of taking certain pharmaceutical drugs. For example, diuretics should be stopped 48 hours before sample collection.
Women should remember that menstruation usually skews the results. For testing, it is better to choose a time before your period or two days after the end of the discharge.
The day before collecting biomaterial, avoid foods with a high content of pigments, alcohol, fatty, smoked foods, sex, and excessive physical and psycho-emotional stress. All this can distort the OAM results.
For analysis, a morning urine sample is collected, optimally its middle part. Before collection, the patient must toilet the external genitalia (bath, shower, wet wipes) .
After the start of urination, it is better to flush the first portion into the toilet, collect the middle portion in a clean, sterile container (optimally in a sterile pharmaceutical container). The minimum volume of urine required for testing is 50 ml. There is a mark on the medicine cup to the level at which it is advisable to fill the container.
In young children, it is often difficult to collect urine for analysis. Therefore, when collecting, you can use small tricks:
- 1Buy special soft polyethylene containers with a sticky edge at the pharmacy. Not all children like this procedure, but for some it is acceptable.
- 2Before picking up, take the baby to the bathroom and turn on the water. A child up to one year old can be breastfed beforehand, and an older baby can be given water to drink. Urination in babies is tied to feeding, so the task can be made easier.
- 3Some children pee several times with intervals between peeings of 10-15 minutes. To collect material from such babies, it is better to prepare several containers so that you can collect the droplets in different dishes without staining them during manipulation.
- 4Before the procedure, you can do a soft, stroking massage in the lower abdomen, in the bladder area.
Factors that distort the results
In order for a urine test to show objective data, it is necessary to eliminate factors that can distort it and complicate the correct diagnosis:
- stress suffered the day before;
- consumption of alcohol, heavy food, sweets;
- taking diuretics and other medications;
- in women - phases of the monthly cycle;
- intense physical activity shortly before the analysis.
The result of the study also depends on the time when the material was received. As a rule, urine is collected from the first urination after waking up. Urine must be sent to the laboratory immediately. Long-term storage can also distort the results of the study.
What should you not do when collecting urine?
When collecting material for clinical urine analysis, it is not recommended:
- 1Use untreated dishes, the contents of a potty, a diaper, a diaper, a plastic bag. This analysis is called “dirty”; it is not suitable for assessing the condition of the urinary system.
- 2Use for analysis stale urine that has stood for more than 3 hours or has been in the refrigerator without a special preservative.
- 3Collect material for OAM after defecation, during menstruation or after sexual intercourse.
- 4Collect material for research during acute inflammatory diseases of the reproductive system, skin around the urethra and vagina (you must warn the doctor about this in advance). It will not be possible to collect such an analysis purely.
- 5Do not use a urinary catheter unless there is an urgent need for it (prostate cancer, prostate adenoma, a bedridden seriously ill patient and other situations that are discussed by the attending physician). When placing a catheter at home, there is a high risk of secondary infection.
The table below presents the main indicators, their standards and interpretation. Clinical urine analysis in women is practically no different from that in men, with the exception of some parameters. These small nuances are noted in the table.
| Index | Decoding | Norm |
| BLd | Red blood cells | 2-3 in the field of view in women (abbreviated as p/z) / Single in men |
| LEU | Leukocytes | 3-6 in p/z for women / Up to 3 - for men |
| Hb | Hemoglobin | Absent (sometimes they write the abbreviation neg - negative) |
| BIL | Bilirubin | Absent (neg) |
| UBG | Urobilinogen | 5-10 mg/l |
| PRO | Protein | Absent or up to 0.03 g/l |
| NIT | Nitrites | Absent |
| G.L.U. | Glucose | Absent |
| KET | Ketone bodies | Absent |
| pH | Acidity | 5-6 |
| S.G. | Density | 1012-1025 |
| COLOR | Color | Light yellow |
Table 1 - Indicators assessed in clinical urine analysis
Physical properties
4.1. Quantity
When assessing the total amount of urine excreted, it is necessary to take into account the possible dietary characteristics of each patient. In an adult who follows a normal diet, daily diuresis ranges from 800 to 1500 ml.
Diuresis directly depends on the volume of fluid drunk. Typically, 60-80% of what you consume per day is eliminated from the body. The normal ratio of daytime to nighttime diuresis is 3:1 or 4:1.
A condition characterized by increased urine output (more than 2000 ml per day) is called polyuria.
A similar phenomenon is observed normally:
- 1If you have drunk a lot over the past day;
- 2In case of nervous excitement or overexertion.
Polyuria can be observed in the following pathological conditions:
- 1Kidney diseases (CKD, stage of resolution of acute renal failure);
- 2 Relief of edema, for example, against the background of diuretics;
- 3Diabetes insipidus and diabetes mellitus;
- 4Nephropathies (amyloidosis, myeloma, sarcoidosis);
- 5Taking certain medications.
The reverse condition is called oliguria. With oliguria, less than 500 ml of urine is excreted per day .
Physiologically it can occur with:
- 1Reduce fluid intake;
- 2Loss of fluid through sweat in the heat;
- 3 Significant physical activity.
It is noted in the following pathologies:
- 1Cardiac decompensation;
- 2 Poisoning;
- 3Excessive loss of water by the body (for example, during profuse diarrhea, vomiting);
- 4Burns;
- 5States of shock;
- 6 Fever of any origin;
- 7 Kidney damage of infectious, autoimmune and toxic origin.
Anuria is a condition in which urine production stops completely . Anuria is typical for:
- 1Initial stage of acute renal failure;
- 2Acute blood loss;
- 3Uncontrollable vomiting;
- 4 Stones in the urinary tract with obstruction of the lumen;
- 5 Oncological diseases accompanied by obstruction and compression of the ureters.
Nocturia is a condition in which nighttime diuresis significantly prevails over daytime . Nocturia is typical for:
- 1Diabetes insipidus and diabetes mellitus;
- 2Many kidney diseases;
- 3BPH.
4.2. Urinary frequency
In addition to the daily amount of urine, pay attention to the frequency of urination. Normally, this process is performed by a person 4-5 times during the day.
Pollakiuria is characterized by frequent trips to the toilet. Observed when:
- 1Drink a large amount of liquid;
- 2Urinary infection.
Olakiuria is the opposite condition to that described above. Characteristic for:
- 1Low intake of fluid into the body;
- 2Nervous reflex disorders.
Strangury is painful urination.
Dysuria is a urination disorder that combines symptoms such as changes in urine volume, frequency and pain. It usually accompanies inflammatory processes in the genitourinary system.
4.3. Color
Is a direct reflection of concentration. In a healthy person, deviations in color from straw yellow to amber are allowed.
The color of urine is also influenced by special substances, the basis of which are blood pigments. A dark yellow color is observed when the amount of coloring substances dissolved in it significantly exceeds the norm. Characteristic of such conditions:
- 1Swelling;
- 2Vomiting;
- 4Burns;
- 4Congestive kidney;
- 5Diarrhea.
If the content of pigment substances is minimal, the shade will be paler. Observed when:
- 1Diabetes mellitus;
- 2Diabetes insipidus.
The dark brown color is explained by an increase in the level of urobilinogen. It is a diagnostic criterion for hemolytic anemia. Urine may turn dark brown when taking sulfonamides.
Dark, practical black color can indicate several conditions:
- 1 Alkaptonuria (due to homogentisic acid);
- 2Acute hemolytic kidney;
- 3Melanosarcoma (obtains this shade due to the presence of melanin).
Urine turns red if it contains fresh blood or red pigments. This is possible with:
- 1Kidney infarction;
- 2Kidney failure;
- 3Damage and trauma to the urinary tract;
- 4Taking certain medications (for example, rifampicin, adriamycin, phenytoin).
The appearance of “meat slop” is explained by the presence of altered blood, which is characteristic of acute glomerulonephritis.
A greenish-brown tint (compared to the color of beer) appears if bilirubin and urobilinogen enter the urine. This deviation from the norm often indicates parenchymal jaundice.
If the shade is rather greenish-yellow, which may indicate the presence of bilirubin alone, and is considered a symptom of obstructive jaundice.
4.4. Transparency
Normally, urine is clear. However, in the presence of pathological components and impurities (proteins, leukocytes, erythrocytes, epithelium, bacteria, salts), it can be cloudy, cloudy and milky.
Several manipulations can be carried out in advance to narrow the range of possible substances that make up the sediment to certain salts.
When, when heated, the test tube with the test material becomes transparent again, we can conclude that it contained urates.
If the same happens upon contact with acetic acid, we can assume the presence of phosphates in the sample. If an identical effect is observed when mixed with hydrochloric acid, then there are calcium oxalates in the urine.
For more accurate data, microscopy of the sediment is performed.
4.5. Smell
The smell of urine is usually specific and not strong. An ammonia odor may appear if there is bacterial contamination of the sample. A fruity smell (of rotting apples) is considered an indicator of the presence of ketone bodies.
4.6. Relative density (SG)
This indicator is considered very important, since it is used to judge the concentration function of the kidneys and its ability to dilute.
The measurement is carried out using a specially designed device - a urometer. During the study, attention is primarily paid to the content of electrolytes and urea, and not to substances with high molecular weight (proteins, glucose, etc.).
Normally, the relative density of the morning urine portion is determined in the range from 1.012 to 1.025. During the day it can fluctuate between 1001 and 1040, therefore, if a patient is suspected of having a decrease in the concentrating ability of the kidneys, the Zimnitsky test is usually prescribed.
Hypersthenuria is an indicator higher than normal . Its cause may be:
- 1 Toxicosis of pregnant women;
- 2 Progressive edema;
- 3Nephrotic syndrome;
- 4Diabetes mellitus;
- 5Use of radiocontrast agents.
Hyposthenuria - decrease in specific gravity . Observed in the following conditions:
- 1Malignant hypertension;
- 2Chronic renal failure;
- 3Diabetes insipidus;
- 4Damage to the kidney tubules.
Isosthenuria is a condition in which the density of urine is equal to the density of blood plasma (within 1010-1011).
UAC
Blood is one of the most important fluids in the body, and it reflects the state of health. Unfortunately, a blood substitute that could save people's lives has not yet been created. The composition of blood is truly unique.
Source: inet-health.ru
Its main components are cells and plasma. The latter has no color and is slightly salty, although it cannot be called just salt water. The cells are responsible for color. They are called red and white blood cells. Each of them has its own function. The most important of them are platelets, leukocytes, and erythrocytes.
Erythrocytes are responsible for nutrition and the respiratory function of all our cells. Leukocytes are always “on guard” of the immune system, fighting viruses and bacteria. Platelets “monitor” various damages and “quickly come to the rescue” during their formation.
Good blood and urine tests in the absence of complaints confirm that the person is completely healthy. If in a blood test the ratio of blood cells is disturbed, their characteristics and quantity change, then you need to look for a pathological focus.
Chemical properties
This is the second group of urine indicators that characterize the patient’s health status.
5.1. Medium reaction (pH)
Normally, urine pH ranges between 5-7. An acidic reaction (pH <5) may result from:
- 1Increased consumption of meat products;
- 2 Metabolic or respiratory acidosis (as a result of various pathological processes), coma;
- 3Acute glomerulonephritis;
- 4Gout;
- 5Hypokalemia.
An alkaline reaction (pH>7) occurs when:
- 1Vegetable diet;
- 2Chronic renal failure;
- 3Metabolic or gas alkalosis;
- 4Hyperkalemia;
- 5Active inflammatory processes in the urinary system.
5.2. Protein Determination (PRO)
Normally, protein is not detected in the urine or an insignificant amount is detected. A condition in which this threshold is exceeded is called proteinuria. It is customary to distinguish several types of proteinuria:
- 1Prerenal proteinuria is associated with pathological processes in the human body that are accompanied by an increase in protein concentration in the blood plasma (myeloma, for example).
- 2Renal - one that is a consequence of damage to the glomerular filter or dysfunction of the renal tubules. The diagnostic criterion for the severity of the pathological process is selectivity - the greater the number of large protein molecules found in secondary urine, the more serious the situation.
- 3 Postrenal proteinuria is a manifestation of inflammatory processes in the reproductive system and surrounding tissues (vulvovaginitis, balanitis, and so on).
- 4Proteinuria can also be physiological, for example, during emotional overload, exposure to cold or sun, in children in a standing position, during long walking or running.
5.3. Determination of glucose (GLU)
Normally, this substance cannot be detected in urine due to its low content. Glucosuria is the name given to a condition in which glucose levels exceed 0.8 mmol/l . This occurs when the so-called renal glucose threshold is exceeded.
That is, when its concentration in the blood exceeds 9.9 mmol/l, it freely passes the barrier and enters the urine. There are the following types of glucosuria:
- 1 Nutritional (large amounts come from food);
- 2Emotional;
- 3Medicinal.
Pathological glucosuria is usually divided into renal (manifests itself in various kidney diseases) and extrarenal, which is considered a consequence of the following diseases:
- 1Diabetes mellitus;
- 2 Thyrotoxicosis;
- 3Pheochromocytomas;
- 4Acute pancreatitis and other diseases of the pancreas;
- 5Itsenko–Cushing's disease;
- 6Liver cirrhosis;
- 7 Poisoning.
5.4. Determination of hemoglobin (Hb)
It is believed that hemoglobin is found in a portion of urine during the rapid breakdown (hemolysis) of red blood cells. Such a process may be infectious, immunological or genetic in nature. Most often, hemoglobinuria is detected with:
- 1Hemolytic anemia;
- 2Transfusion of incompatible blood;
- 3Internal injuries (crash syndrome);
- 4Severe poisoning;
- 5Direct damage to kidney tissue.
Hemoglobinuria is dangerous because it is an impetus for the development of acute renal failure.
5.5. Determination of ketone bodies (KET)
Ketonuria is a special indicator of urine analysis, which reflects the failure of metabolic processes occurring in the body . In this case, the following substances are detected: acetone, beta-hydroxybutyric, acetoacetic acids. Ketonuria occurs against the background of:
- 1Diabetes mellitus;
- 2Carbohydrate starvation, diets;
- 3 Severe toxicosis (more often in children);
- 4Dysentery;
- 5 Severe irritation of the central nervous system;
- 6Hyperproduction of corticosteroids.
5.6. Determination of bilirubin (BIL)
Bilirubinuria is a pathological condition in which unchanged bilirubin is detected in the urine . When the mechanisms that utilize bilirubin fail, the kidneys take on part of the work. Bilirubinuria is typical of many liver diseases:
- 1 Cirrhosis;
- 2 Hepatitis;
- 3 Jaundice (parenchymal and mechanical);
- 4Cholelithiasis.
5.7. Determination of urobilin bodies (UBG)
Urobilinuria occurs when the liver does not function properly. However, intestinal pathology (where this substance is formed) and processes leading to the breakdown of red blood cells also contribute to the appearance of urobilinogen in the urine.
A high content of urobilinogen bodies in the sample (UBG in the analysis form) is detected when:
- 1Hepatitis;
- 2Sepsis;
- 1Hemolytic anemia;
- 4 Cirrhosis;
- 5 Intestinal diseases (inflammation, obstruction).
Do reference values depend on age and gender?
All etiological factors for changes in the number of blood cells in urine are divided into physiological and pathological. The first group of factors is natural and depends on the patient’s condition. The analysis in both situations is carried out the same way.
Below are the physiological reasons why the number of red blood cells in urine changes:
- prolonged exposure to high ambient temperatures;
- drinking alcohol;
- severe stress;
- physical exercise;
- use of spices and herbs.
With a physiological increase in the number of red blood cells, the shade of urine does not change, so this change remains unnoticed by humans.
Pathological factors can be divided into 5 groups:
- kidney pathologies;
- diseases of the urinary organs;
- pathologies of the reproductive system;
- hematological disorders;
- other deviations.
With age, the content of red blood cells increases: since due to old age, capillary permeability increases, inflammation becomes more frequent, and blood clotting decreases. If only 3 blood cells are detected in the urine, the doctor should prescribe repeated tests.
Microscopic examination of sediment
Microscopic examination of organized and unorganized urine sediment is of great importance in diagnosis. For this purpose, the laboratory technician lets the resulting sample sit for about two hours, then centrifuges it, drains the liquid, and examines a drop of sediment under a microscope.
At low magnification, the cylinders within the field of view are counted, and at high magnification, leukocytes, erythrocytes and other cellular elements are counted.
Counting the number of cellular elements in a material greatly facilitates the use of Goryaev’s camera.
6.1. Red blood cells (BLD)
Normally, there are red blood cells in the urine, but their number is limited to one cell in the field of view in men and up to three in women).
Hematuria is a condition in which more red blood cells are found in the urine. There are macrohematuria (the presence of blood clots can be determined with the naked eye) and microhematuria (the presence of red blood cells can only be detected using a microscope).
Figure 1 - Changed erythrocytes in urine under a microscope, native preparation. Source Masaryk University (https://is.muni.cz/do/rect/el/estud/lf/js15/mikroskop/web/pages/zajimave-nalezy_en.html)
In addition, glomerular (renal) hematuria is distinguished, which manifests itself in kidney diseases of various origins, medicinal and toxic damage to the renal tissue, and non-glomerular, which is associated with the inflammatory process, injuries and oncological diseases.
Figure 2 - Unmodified erythrocytes (native preparation, red arrow indicates erythrocyte and leukocyte). Source Masaryk University
6.2. Leukocytes (LEU)
In a healthy man, leukocytes in the urine are represented by a small number of neutrophils (up to three), in women there are slightly more of them (up to six).
An increase in the level of white blood cells in the urine is called leukocyturia. This always indicates inflammatory processes in the kidneys or urinary tract, such as:
- 1Pyelonephritis;
- 2Glomerulonephritis;
- 3Kidney tuberculosis;
- 4Cystitis;
- 5Urethritis;
- 6 Fever.
If among all the cells there are noticeably more eosinophils, then they talk about the allergic genesis of the disease, if there are lymphocytes - about the immunological one.
Figure 3 - Leukocytes in urine under a microscope
6.3. Epithelium
Normally, microscopy reveals up to 5-6 cells. However, the elements should be distinguished from each other, since they reflect different clinical manifestations:
- 1Squamous epithelium enters the material from the external genitalia. Often observed with urethritis in men, in poorly collected samples in women.
- 2Transitional epithelium is part of the mucous membrane of the urinary tract. Found in cystitis, neoplasms, pyelitis.
- 3Renal epithelium, present in large quantities in TAM, indicates the following conditions: acute and chronic kidney damage, intoxication, fever, infection.
6.4. Cylinders
These are protein or cellular elements originating from the tubular epithelium.
- 1Hyaline (protein) appear when:
- dehydration of the body;
- nephropathy in pregnant women;
- fevers;
- poisoning with salts of heavy metals.
- 2Waxy (protein) speaks of:
- nephrotic syndrome;
- amyloidosis.
- 3Cell casts can indicate problems of a very wide etiology and are a direct indication of more detailed analyzes.
6.5. Slime
Normally found in small quantities. At higher levels, mucus may indicate the following diseases:
- 5Urethritis;
- 2Prostatitis;
- 4Cystitis;
- 4Kidney stone disease;
- 5Incorrect sample collection.
Video Photo Tables
| Index | Decoding | Norm |
| BLd | Red blood cells | 2-3 in the field of view in women (abbreviated as p/z) / Single in men |
| LEU | Leukocytes | 3-6 in p/z for women / Up to 3 - for men |
| Hb | Hemoglobin | Absent (sometimes they write the abbreviation neg - negative) |
| BIL | Bilirubin | Absent (neg) |
| UBG | Urobilinogen | 5-10 mg/l |
| PRO | Protein | Absent or up to 0.03 g/l |
| NIT | Nitrites | Absent |
| G.L.U. | Glucose | Absent |
| KET | Ketone bodies | Absent |
| pH | Acidity | 5-6 |
| S.G. | Density | 1012-1025 |
| COLOR | Color | Light yellow |
Additionally
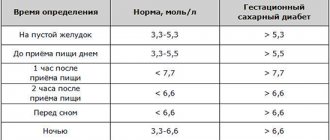
In addition to the UAC and OAM, there are other tests that allow you to assess your health status using blood or urine. So, we are talking about glucose tolerance analysis, which is very important for those who are at risk for diabetes.
If various infectious diseases are suspected, an antibody test is prescribed.
Genetic screenings are also important, especially for those planning a pregnancy. With their help, you can determine which hereditary pathologies threaten a woman and her future children.
Any tests are taken when there is really a need for them, and not just like that. Quite often you can hear the phrase that tests “do not cure.” Symptoms and complaints are needed.
As for urine, which, as we have already mentioned, is nothing more than filtered blood, it is quite easy to track the functioning of the kidneys. For example, the Zimnitsky test is used for this purpose, when the patient needs to collect daily urine.