DERMATOSES
(
dermatosis
, singular; Greek derma, dermat[os] skin + -osis; synonym:
skin diseases
, obsolete -
rashes, rashes
) - a collective term denoting various congenital and acquired pathological conditions of the skin and its appendages; This concept includes skin changes of various origins: dystrophic, inflammatory, infectious, hereditary, etc.
The term “dermatoses” includes both individual nosole, forms, and group concepts (for example, “dermatitis”, “mycoses”, “dermatozoonoses”, etc.). Temporary symptomatic changes in the skin that do not have an independent wedge, meaning and do not require independent treatment, observed in some infectious diseases (typhoid fever, scarlet fever, measles, jaundice, etc.), are not included in the concept of “dermatoses”.
In modern literature, approx. 2 thousand D. At the same time, the wedge, variants of the same D. often have independent traditional names (for example, manifestations of infiltrative-suppurative trichophytosis - parasitic sycosis, kerion Celsi, etc.).
According to P.V. Kozhevnikov (1970), the diversity of dermatols and pathologies is due to the following factors. 1. Anatomical-physiol, the complexity of the skin, formed by a number of morphol, structures (see Skin), although connected with each other, but can have an independent patol, condition, in connection with which diseases of the sweat glands can be distinguished - anhidrosis (see) , hydrocystoma (see), hyperhidrosis (see), dyshidrosis (see), prickly heat (see), etc.; diseases of the sebaceous glands - acne (see), tumors and nevi of the sebaceous glands; hair diseases - see Hair, table. Nail diseases - see Nails. 2. The ability to observe the dynamics of skin lesions with the naked eye and using a number of research methods, which facilitates the identification and description of wedges and variants. 3. Features of the structure and functional state of the skin in various parts of the human body, in connection with which it is possible to identify diseases characteristic of the folds of the skin, scalp, skin of the palms and soles, etc. 4. The variety and abundance of environmental factors affecting the skin.
General information
Dermatoses in adults are represented by a wide group of heterogeneous diseases of the skin/its appendages of different origins (allergic, infectious, immune, hereditary, dystrophic, etc.), caused by external/internal causes or combined etiological factors.
In fact, “dermatosis” is a collective term denoting various acquired/congenital pathological conditions of the skin and skin appendages. At the same time, this term includes both group concepts (“dermatitis”, “dermatozoonoses”, “pyoderma”, “toxicoderma”, “mycoses”, “photodermatoses”, “keratoses”, “psychogenic skin diseases”, etc.) and individual nosological forms. About 2 thousand dermatoses are presented in the literature, and often variants of the clinical course of one dermatosis have independent names. In the structure of dermatoses in adults, the most common are atopic dermatitis , allergic dermatitis , eczema , psoriasis , pyoderma , urticaria , vitiligo , acne conglobata , seborrheic dermatitis , neurodermatitis , furunculosis , keratosis pilaris , ichthyosis , alopecia areata , palmoplantar keratoses derma , scabies , mycoses (microsporia, trichophytosis, mycoses of the feet), viral dermatoses (herpes simplex/shingles). Relatively rare dermatoses include elastosis (skin atrophy) and, in particular, solar elastosis, which is accelerated degenerative changes in the connective tissue of the skin (collagen/elastic fibers) that develop under the influence of ultraviolet rays (skin photoaging). Occupational dermatoses are also relatively rare.
Data on the prevalence of certain dermatoses among the population, gender indicators, and the proportion of specific nosological forms vary over an extremely wide range.
Over the past decade, there has been an increase in the proportion of clinical chronic dermatoses, forms with a severe/recurrent course, resistant to standard methods of therapy, which contributes to a prolongation of the period of disability and an increase in cases of disability. The chronic course of the vast majority of chronic dermatoses causes psychosocial maladaptation in patients of varying degrees of severity, leading to a decrease in quality of life. Moreover, in many patients with chronic dermatoses, the lack of remission and the presence of constant irritation in the form of disturbing itching forms an additional pathogenic complex, leading to a disturbance in the psycho-emotional state and exhaustion of the nervous system. Let us briefly consider only some groups of dermatoses.
Infectious dermatoses . Patients with skin infections constitute the largest group of dermatological patients. The causative agents of infectious dermatoses may include viruses, bacteria, and fungi. A common feature of skin infections is the important role of the state of the immune system, which largely determines their course. Infectious dermatoses include pyoderma , hidradenitis , vesiculopustulosis , epidemic pemphigus of newborns , streptococcal impetigo , cellulitis , paronychia , erysipelas , boils , etc.
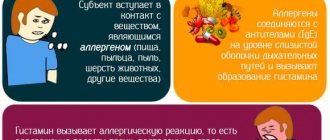
Pruritic dermatoses are a group of skin diseases caused by primary, severe universal/limited skin itching and scratching (excoriation), to which the skin responds with the development of lichenification/lichenoid papules. In most cases, itchy dermatosis is a manifestation of an allergic reaction to allergens, which can be a variety of factors (animals, cosmetics, food/plant allergens, stress, etc.). Often this group of diseases is called allergic dermatosis (allergic dermatosis), since allergic dermatosis develops with repeated contact with an allergen to which the patient is hypersensitive. The most common pruritic dermatoses include atopic dermatitis , psoriasis , prurigo , chronic urticaria , neurodermatitis , pityriasis rosea , allergic contact dermatitis , eczema , scabies , seborrheic dermatitis , etc.
Bullous dermatoses (syn. blistering dermatoses) are represented by a group of skin diseases of non-infectious origin, differing in etiopathogenesis, clinical course and pathohistological changes. For bullous dermatitis, a characteristic feature is the formation of monomorphic rashes in the form of blisters or combined with a polymorphic rash. Bullous dermatoses are represented by such nosological forms as impetigo , true pemphigus , burns , bullous zpidermolysis , contact dermatitis , reactions to insect bites, benign chronic familial pemphigus , pemphigoids , dermatosis herpetiformis , bullous drug rash , autoimmune pemphigus , etc. Bullous dermatosis are characterized by a severe course, and in some of them, in the absence of adequate treatment, there is a high risk of death.
Dermatosis: causes and definition
Dermatosis can occur as an independent disease, or it can be a companion to a certain disease. There are many types of dermatosis. They can be triggered by various factors, which, in turn, can be located inside and outside the body.
Internal causes of dermatosis, which occur as a reaction to various types of diseases, as well as when the immune system malfunctions:
- Various types of allergies.
- Hereditary predisposition.
- Drug poisoning.
- Gastrointestinal diseases.
- Hormonal imbalances.
- Inflammatory processes.
- Infectious diseases.
- Worm infestation.
- Diseases of the endocrine system.
- Diseases of blood vessels and blood.
- Prolonged fevers.
- Stress, diseases of the nervous system.
External signs appear under the influence of external factors on the body:
- Contact with aggressive chemical components.
- Cosmetical tools.
- Contact with components and objects containing allergens.
- Household chemicals.
- Stinging and poisonous plants.
- Insect bites.
- Mechanical influences.
- Occupational allergens.
As we see, there are many reasons for the appearance of dermatosis. Each causes a certain type, which determines the clinical picture of the disease, distinctive signs and often treatment methods.
Symptoms of dermatosis
Clinical features of the development and course of itchy dermatosis photo, analysis of its symptoms, allow us to distinguish three groups of signs of diseases:
- Objective (main) skin manifestations. Various types of rashes: erosion, blisters, pustules, plaques, spots, crusts, ulcers and others. Allergic rashes, redness, peeling, and so on.
- Subjective skin sensations. These include: burning, itching, decreased sensitivity: numbness, pain.
- Additional signs. Weakness, fever, decreased body resistance.
Forms of dermatosis
Based on the combination of factors for the appearance of dermatosis, the disease is divided into various groups:
- Pyoderma. Characterized by skin rashes in the form of pustules.
- Viral. They occur when the body is infected with viral pathogens.
- Mycoses. Appear when the body is infected with fungi.
- Itchy allergic dermatoses.
- Skin diseases transmitted genetically.
- Dermatoses caused by parasitic diseases.
- Skin lesions in cancer (skin tumors).
According to the totality of development processes and main signs, according to international qualifications, dermatosis is divided into groups:
- Bullous signs. Blisters appear on the skin (from the English bull - bubble).
- Eczema, weeping and dry.
- Papulosquamous signs. They are characterized by the formation of keratinized scales and rashes on the skin. These include psoriasis.
- Skin infections.
- Erythema and urticaria. Characterized by redness of the skin and the appearance of a rash.
- Radiation injuries.
- Diseases of the skin appendages - nails, hair.
- Other types of dermatoses.
Pathogenesis
The pathogenesis of dermatoses varies extremely depending on the group of dermatoses and nosological forms, and it is not possible to describe them within the scope of the article. It should only be pointed out that a significant role in the development of dermatoses is played by an allergic reaction of immediate/delayed type, autoimmune disorders, toxic damage to the skin, violation of the integrity of the skin, infection of the skin/metastasis of an infectious agent into it, degenerative changes in collagen/elastic fibers of the skin, neurogenic mechanisms, etc. .
Diagnostics
To identify dermatosis and determine its type, a consultation with a dermatologist is required. The doctor usually does:
- A thorough examination of the patient, visual assessment of the characteristics of the rash, as well as other signs of the disease.
- Anamnesis collection. The doctor always asks whether the patient has had allergies before, and whether other family members and close relatives have dermatological allergic diseases.
- Skin scraping for microscopic examination and biopsy.
- Blood and urine tests.
Typically, diagnosing allergic dermatoses is not difficult. Most often, the doctor makes a preliminary diagnosis during the initial appointment.
Classification
Several classifications of dermatoses have been proposed, based on various characteristics. Below is a simplified version of the classification of dermatoses, according to which they are distinguished:
- Itchy dermatoses - atopic dermatitis , psoriasis , prurigo , chronic urticaria , neurodermatitis , pityriasis rosea , allergic contact dermatitis , eczema , scabies , seborrheic dermatitis , etc.
- Bullous dermatoses - true pemphigus (vegetative, erythematous, vulgaris, foliate, Brazilian), pemphigoid (bullous, recurrent), dermatoses herpetiformis (herpes of pregnancy, Dühring's dermatosis herpetiformis.
- Allergic dermatoses - atopic, toxic-allergic, contact dermatitis , erythema .
- Infectious dermatoses (bacterial, viral, fungal) - pyoderma , hidradenitis , vesiculopustulosis , epidemic pemphigus of newborns, streptococcal impetigo , paronychia , erysipelas , mycoses , etc.
- Parasitic dermatoses - caused by parasitic insects (scabies, leishmaniasis, cysticercosis).
- Occupational dermatoses - skin pathologies caused by contact with various irritating, allergenic and industrial environmental factors (fiberglass, dust, acids, alkalis) - toxicoderma , epidermoses , folliculitis , dermatitis , eczematous manifestations , vasculitis , porphyria , melasma , vitiligo , lichen , occupational eczema , paronychia , onychia , burns , photodermatoses , urticarial rashes , Quincke's edema , dermatoconiosis , etc.
Classification of allergic diseases
There are several types of allergic itching dermatoses. Among them, doctors highlight:
- Allergic dermatitis and diathesis.
- Toxicoderma.
- Eczema.
- Atopic dermatitis.
- Hives.
- Strophulus.
- Exudative erythema.
- Stevens-Jones syndrome.
- Lyell's syndrome.
Allergic dermatoses are characterized by an acute onset. They are prone to a chronic course, regardless of the form of human contact with an individually significant allergen.
Causes
Dermatoses are based on polyetiological factors that act as triggers of pathological processes of the skin/skin appendages, which are conventionally divided into 2 groups: internal (endogenous) and external (exogenous).
The group of endogenous factors includes:
- Hereditary predisposition/genetic defect.
- Local infection of various locations - in the nasopharynx (tonsils, maxillary sinuses, gallbladder/bile ducts, kidneys ( pyelonephritis ), etc.
- Chronic diseases of internal organs (liver, intestines, kidneys), which carry out processes of neutralization/removal of toxins from the body.
- Hypovitaminosis (A, groups B, C and P).
- Functional/organic circulatory disorders.
- Lymph circulation disorders.
- Functional/organic lesions of the peripheral (neurovegetative disorders) and central nervous system.
- Disorders of the function of the endocrine glands (thyroid gland, adrenal glands, gonads).
- Genetic defect, hereditary predisposition.
- Immunosuppressive conditions.
- Diseases of the hematopoietic system.
The group of exogenous factors includes:
Physical/chemical/biological exposure factors, environmental factors (mechanical irritants, low/high temperature, electric current, ionizing radiation, ultraviolet rays, food products, chemicals, drugs, infectious agents, etc.).
As a rule, the development of dermatosis is caused by a combination of several factors: the action of a trigger, a decrease in local skin protection, insufficient immune response to the influence of an aggressive factor, etc. In some cases, even an isolated impact (burn/frostbite) can provoke a skin disease.
Symptoms
Symptoms of dermatosis depend on the group of dermatoses and the specific nosological form, and it is not possible to give an exhaustive description of them within one article. The general symptom of most dermatoses is the presence of primary/secondary various morphological elements of the rash - spot, papule, tubercle, node, vesicle, bubble, pustule, blister, excoriation, crack, scales, crust, ulcer, scar, pseudoleukoderma (discolored spots on the skin in the area localization of resolved rashes). At the same time, certain nosological forms are characterized by the same type of rash, and for some there is their diversity or staged polymorphism. Also, a number of dermatoses are characterized by the specific localization of rash elements, the number of rash elements (multiple/single), the time period of their appearance, the uniformity of distribution, the simultaneous appearance or spread over time, the merging of rash elements, and the background of the skin.
Symptoms of dermatosis often manifest themselves as itching (pruritic dermatoses), against which secondary foci of infection appear due to scratching and colonization by various pathogenic/opportunistic microflora. In this case, bacteria/fungi can act as triggers that provoke exacerbation of chronic dermatoses. In addition to local manifestations, a number of dermatoses may also cause the general condition of the patient to suffer (low-grade fever, headaches, general malaise), and there may be changes in the lymphatic system and blood.
Allergic dermatoses are one of the groups of dermatoses often encountered in medical practice, the representatives of which include atopic dermatitis , eczema , contact dermatitis , neurodermatitis , and urticaria . The clinical picture of dermatoses in this group is characterized by significant severity of inflammatory changes in the skin. Thus, allergic dermatosis manifests itself with various types of allergic rashes (erythematous, vesicular/papular elements) on the skin of almost any part of the body. Elements of the rash usually develop against the background of erythema and are accompanied by a feeling of heat, burning and disturbing itching. An allergic rash is characterized by a weakly expressed polymorphism of rashes (scales, erosions, vesicles, papules, crusts), and directly in the affected areas there is swelling, bright hyperemia, weeping and the formation of scales-crusts/crusts in the future. With this pathology, acute inflammatory changes in the skin develop suddenly and increase in intensity extremely quickly, causing physical/psychological discomfort (photo below).
Allergic dermatitis completely/quickly regresses after eliminating contact with the allergen. At the same time, the risk of relapse of allergic contact dermatitis upon repeated contact with the allergen is quite high and develops quickly.
Blistering dermatoses are characterized by an undulating chronic course. Let us consider only the symptoms of true pemphigus vulgaris, which is characterized by monomorphism of rashes, the appearance on visually unchanged skin/mucous membranes of the nasal/oropharynx, genitals, red border of the lips of various sizes of intraepidermal blisters with serous contents (Fig. below).
Patients experience pain when swallowing saliva, eating and talking. A characteristic symptom is the appearance of a specific odor from the mouth and drooling (hypersalivation). As a rule, the mucous membrane is initially affected, and later (after 3-6 months) the process spreads to the skin. At the same time, the appearance of blisters on the mucous membranes often goes unnoticed due to their rapid opening, and in their place painful, long-term non-healing erosions form. Blisters on the skin also persist for a short time, and some of them may shrink into crusts. Characteristic is Nikolsky's symptom , manifested by the separation of layers of the epidermis with minor mechanical impact. With vulgar pemphigus , erosions with a shiny, moist surface of a bright pink color, and their feature is a tendency to peripheral growth and the risk of the formation of extensive lesions (generalization of the skin process) with the addition of a secondary infection, deterioration of the general condition, the development of intoxication and, if left untreated, fatal outcome. pseudoleukoderma often develops . In general, bullous dermatitis is characterized by a severe course.
Dermatosis of pregnant women
Alas, in recent years, pregnancy dermatosis has been diagnosed quite often, which in the vast majority of cases appears in the third trimester. This dermatosis of pregnant women is characterized by the following forms:
- papillomas;
- herpes;
- skin itching;
- strip;
- itchy folliculitis;
- hives;
- papular dermatitis;
- autoimmune dermatitis;
- prurigo;
- impetigo.
Women who often experienced skin rashes even before pregnancy should be especially careful. The fact is that the likelihood of recurrence of the disease during gestation increases several times. The main reason should be changes in the activity of the immune system , active synthesis of bile acids and hormonal disorders. However, after the end of childbirth, the situation may change noticeably, as a result the disease may begin to regress. Despite the fact that dermatosis in pregnant women is temporary, it should still be constantly under medical supervision.
During pregnancy
Dermatoses of pregnancy are represented by a group of specific skin diseases ( atopic eruptions of pregnancy , pemphigoid of pregnancy , polymorphic dermatosis of pregnancy and intrahepatic cholestasis of pregnancy ), which arise during gestation and resolve spontaneously after childbirth.
Let's consider polymorphic dermatosis of pregnancy, which is a self-limiting benign inflammatory disease of the skin, which is characterized by intense itching and a polymorphic rash (urticarial papules/plaques, small vesicles). The incidence rate varies between 0.45-1.0%. At the same time, about 40% of cases occur in first-time women, 30% of cases - in women with a second pregnancy, and 15% of cases - in women with a third pregnancy. Polymorphic dermatosis in most cases occurs in the 3rd trimester of pregnancy, the incidence of the disease in the 1st and 2nd trimester is significantly lower, and in the postpartum period polymorphic dermatosis is extremely rare.
Primary rashes are located mainly on the skin of the abdomen, often on the surface of “stretch marks” (stretch marks). At the same time, the skin of the peri-umbilical area is not affected. Less commonly, rashes spread to the breasts, lower back, buttocks, thighs and upper limbs. Damage to the mucous membranes/skin of the scalp, face, palms, and soles is uncharacteristic. Subsequently, the primary elements evolve into scales/crusts, and later into unstable hypopigmented spots. There is no scarring process (photo below).
The duration of the rash varies between 3-6 weeks, and its maximum severity is observed in the first week of the rash. Itching is moderate to severe, with virtually no excoriation. As a rule, the rash resolves on its own, and there are no associated complications for the fetus and the woman. Children do not develop rashes after birth.
Treatment is carried out by prescribing topical steroid drugs of groups II-V ( Laticort , Flucinar , Lorinden , Oxycort ), antipruritic lotions (Calamine lotion "Sarna") and cool compresses.
Pruritic dermatosis
The concept of pruritic dermatosis combines a large variety of dermatoses. They are in many cases caused by allergic irritants, leading to unbearable itching and rash. The main representatives of pruritic dermatosis include: contact dermatitis, atopic dermatitis, prurigo (prurigo), vesicular dermatosis, polymorphic observed in pregnant women, herpes of pregnant women and others. Let's consider individual types:
Prurigo (prurigo)
Prurigo, popularly called prurigo, is one of the representatives of pruritic dermatosis. It is divided into two groups:
- Prurigo Hyda. A rare disease that affects most women between 30 and 40 years old. Skin disease occurs due to metabolic, hormonal and intoxication failures. In this case, rashes of small pimples appear on the body, remaining on the skin for a very long time. Treatment of the disease takes a long period.
- Prurigo Hebra. This form of pruritus mainly affects children under one year of age. Rashes with this disease resemble urticaria, with characteristic large pimples. The skin on them thickens and cracks. Complications caused by infection often occur when scratching. Thickening of the lymph nodes in the groin occurs.
Allergic contact dermatitis
Allergic dermatitis is characterized by contact with allergic irritants, upon interaction with which the disease develops. The mechanism of the disease is simple; contact with an irritant triggers an allergic reaction, which consists of skin rashes with characteristic symptoms: burning and unbearable itching.
The rashes are small papules grouped into plaques. They can be located on the neck, elbows and knees, as well as on the genitals, in the anus. The skin becomes dry and flaky. An unbearable itching appears, which becomes stronger at night.
When scratching, wounds appear on the skin, which begin to bleed and crusts appear on them. With dermatosis in children, rashes can spread throughout the body. The first stage of treatment will be to identify the irritant, otherwise it is impossible to remove the symptoms.
Blistering dermatosis
Itchy dermatoses include blistering dermatoses, in which blisters of various shapes appear on the non-inflamed surface of the skin, accompanied by itching. Their appearance can be explained by skin separation. It begins to exfoliate as a result of water getting between the layers of the epidermis, which seeps from the intercellular space or through the capillaries. The fluid may be clear or mixed with blood and pus. The main causes of blistering dermatosis may be:
- Thermal or sunburn.
- Burns from chemicals.
- The effect of cold on the skin is frostbite.
- Autoimmune skin lesions.
- Toxidermy (drug poisoning).
- Bacterial infections.
- Eczema.
- Scabies.
- Prickly heat.
- Other.
In some cases, the blisters burst, the liquid flows out, and erosions form, which become covered with crusts, under which the skin regenerates, and painful cracks often form.
Treatment begins with local therapy, which is supplemented with drugs depending on the reasons that caused the appearance of blistering dermatosis: antiviral, antibacterial, anti-inflammatory and wound-healing drugs. Self-medication is dangerous. You need to go to the clinic.
Polymorphic dermatosis in pregnant women
Women in the third trimester of pregnancy in some cases develop polymorphic dermatosis. This is the body’s response to hormonal imbalance caused by its restructuring. Papules appear on the chest and abdomen, which begin to itch and itch unbearably. Dermatosis develops within two weeks and disappears on its own after ten days.
Antihistamines and sedatives are taken internally. Take medications only under medical supervision.
Herpes in pregnant women
This disease has nothing in common with herpes simplex. The disease is autoimmune in nature and occurs exclusively in pregnant women. The first signs appear at different stages of pregnancy or a few hours after birth. They are localized in the umbilical region, and quickly move throughout the abdomen, moving to the thighs, chest, palms and feet.
The rash appears in the form of papules, which transform into blisters. There is unbearable itching. Over time, the disease disappears, but a recurrence can occur after a second pregnancy or during any menstruation. Childbirth usually occurs earlier than the specified period, but the child’s life is not in danger.
Mechanism of development of dermatosis
The human skin represents a powerful defense of the body from external influences, which can be different:
- Physical effects on the skin: heat, cold, friction, shock, radiation. When they act on the skin, damage appears: burns, frostbite, calluses, bruises, degenerative changes.
- When exposed to chemical elements, the skin is exposed to allergic conditions: rashes, spots, redness of the skin.
- When exposed to bacteria, pustular rashes and skin tuberculosis appear on the skin.
- Viral infections cause skin diseases: shingles, warts, molluscum contagiosum infection.
- When fungal intoxications occur, keratomycosis occurs, represented by damage to the nails and hair, mycoses.
- The parasitic form is represented by dermatosis caused by scabies mites.
- With endogenous forms, various types of dermatosis occur depending on the disease.
- Often the appearance of dermatosis is provoked by a strong emotional state, stress.
- Failure to maintain proper skin hygiene.
The mechanism of occurrence and progression of dermatoses is quite complex; depending on external and internal causes, one or another form of the disease is formed. An important role in its formation is played by:
- Disruption of the nervous and hormonal systems.
- Hereditary predisposition.
- Disturbance in the functioning of the circulatory system.
- Autoimmune processes.
Therapy of dermatoses
When treating dermatosis, the main task is to identify and eliminate the substance that causes the disease. Until the pathogen is identified, any treatment is meaningless. Therapy for itchy dermatoses is carried out in two stages: general and local. Treatment includes symptomatic, pathogenetic and etiological therapy.
Local therapy is symptomatic treatment, that is, elimination of the symptoms of the disease. For this purpose, ointments, aerosols, lotions and other drugs are used that remove inflammation and relieve itching. Allergic dermatoses are treated with antihistamines caused by antimicrobial viruses.
Physiotherapy and sanatorium treatment are good remedies. Skin diseases caused by itchy dermatoses cause inflammatory processes. Glucocorticosteroids are used to block them. All prescriptions prescribed by the doctor must be strictly followed. Self-medication is strictly prohibited!
Similar articles
Diet
Hypoallergenic diet
- Efficacy: therapeutic effect after 21-40 days
- Timing: constantly
- Cost of products: 1300-1400 rubles. in Week
Diet for skin diseases
- Efficacy: therapeutic effect after a month
- Time frame: three months or more
- Cost of products: 1400-1500 rubles per week
Diet for dermatitis
- Efficacy: Therapeutic effect after 3 weeks
- Timing: Constantly
- Cost of products: 1300-1390 rubles per week
Diet for psoriasis
- Efficacy: healing effect
- Timing: constantly
- Cost of products: 980-1150 rubles per week
In the complex therapy of dermatoses, rational dietary nutrition is the most important method of treatment. This primarily applies to allergic/pruritic dermatoses, but is also important for dermatoses of other groups. For this purpose, Diet for Dermatitis , Hypoallergenic Diet , Diet for Skin Diseases , Diet for Psoriasis , and so on may be prescribed.
Since almost any dermatosis has an allergic component, it is recommended to exclude from the diet foods that have a high sensitizing activity, contain histamine or contribute to its production (chocolate, cow's milk, strawberries, coffee, cocoa, orange juice, hard cheeses, smoked meats, tomatoes, hazelnuts , tuna, herring) and artificial food additives.
In case of atopic / seborrheic dermatitis, all easily digestible carbohydrates (jam, sugar, sweet pastries, preserves, confectionery, condensed milk, sweets, honey) are subject to restriction. Also excluded are smoked meats, sausages, seafood, rich broths, red meat, marinades/sauces, canned fish/meat, seasonings (mustard, horseradish, vinegar, ketchup, mayonnaise), pickled vegetables, mushrooms, spicy dishes, salt, sauces, animal fats. , sweet drinks and alcoholic drinks.
For a number of dermatoses, it is necessary to exclude specific groups/types of foods from the diet, for example, for bullous dermatoses ( Dühring's dermatitis herpetiformis ) - exclusion of foods containing glutin and iodine. A particularly strict diet should be followed for chronic recurrent dermatoses during exacerbation.
Prevention
There is no specific prevention. For each specific nosology, there are specific preventive measures, for example, for atopic dermatosis - avoidance of triggers (provoking factor) - contact/food allergens, aeroallergens; for mycoses - compliance with hygiene rules in the team/family, carrying out disinfection measures in public places (hotels, hairdressers, sports complexes, baths, dormitories); for infectious dermatoses - limit contact with persons who are carriers of skin diseases of infectious origin; for industrial dermatoses - use of personal protective equipment when in contact with aggressive substances at work, and so on.
List of sources
- Kirichenko I.M. Modern approaches to the treatment of infectious skin diseases. Cons. Med. 2006; 8 (1): 8-10.
- Korotkiy N.G., Taganov A.L., Tikhomirov A.A. Modern external therapy of dermatoses (with elements of physiotherapy). Ed. N. G. Korotkoy. Tver: Provincial Medicine, 2001.
- Albanova V.I., Nefedova M.A. Acquired epidermolysis bullosa: difficulty of diagnosis. Bulletin of Dermatology and Venereology 2021, No. 2; With. 65-72.
- Clinical dermatovenerology. Guide for doctors in 2 volumes. Ed. Yu. K. Skripkina, Yu. S. Butova. M.: GEOTAR-Media, 2009. T. 1, 720 p. T. 2, 928 p.
- Federal clinical guidelines. Dermatovenereology 2015: Skin diseases. Sexually transmitted infections. — 5th ed., revised, and additional. - M.: Business Express, 2021. - 768 p.
Principles of diagnosis and treatment
When diagnosing
D. it is necessary to establish the nature of the morphol, elements and assessment of the rash as a whole: its monomorphism or polymorphism (true - the presence of various primary elements or false - due to secondary elements developing from one primary), prevalence, symmetry, nature of the boundaries, features of the localization of the rash, its connection with nerves or vessels, the location of the elements of the rash (disseminated, grouped, prone to fusion, etc.). Methods used to diagnose D. - see Dermoscopy.
Treatment
in patients D. should be general (according to etiological, pathogenetic characteristics, symptomatic) and local. External pharmacological agents have a symptomatic effect - anti-inflammatory, resolving, keratolytic, antipruritic, destructive (cauterizing), stimulating regenerative processes, depigmenting, repigmenting, anti-sclerosing, as well as etiological - disinfectant, antifungal, antiparasitic. With the help of special dosage forms (solutions, lotions, powders, shaken suspensions, ointments, jellies, creams, liniments, pastes, varnishes, patches, soaps, adhesives), it is possible to dose pharmacol, agents, regulate the depth of their penetration into the skin, and also provide a symptomatic therapeutic effect due to physical. properties of the dosage forms themselves. Diet therapy, physiotherapy, and sanatorium-resort treatment are widely used for both curative and preventive purposes.
For the history of the study of skin diseases, congresses of dermatologists, etc., see Dermatology.
See also articles devoted to individual skin diseases (eg, Acrodermatitis, Folliculitis, Eczema, etc.).
Bibliography:
Kozhevnikov P.V. General dermatology, L., 1970, bibliogr.; Kr and Nevsky A.M. Multi-volume guide to dermatovenerology, ed. G. T. Pavlova, vol. 1-3, M., 1959-1964; PopovL. X. Synthetic dermatology, trans. from Bulgarian, Sofia, 1963; Raben A. S. and Antonev A. A. Professional dermatology, M., 1975, bibliogr.; Skripkin Yu. K., Somov B. A. and Butov Yu. S. Allergic dermatoses, M., 1975, bibliogr.; Studnitsin A. A., Stoyanov B. G. and Sharapova G. Ya. Skin diseases in children, M., 1971, bibliogr.; Torsuev N. A. et al. Allergic itchy dermatoses, Kyiv, 1973; BohnstedtR. M. Krank-heitssymptome an der Haut in Beziehung zu Storungen anderer Organe, Stuttgart, 1963; G ert 1 er W. Systematische Dermatologie und Crenzgebiete, Bd 1-3, Lpz., 1970-1973.
V. I. Samtsov.