Malabsorption syndrome or malabsorption is a complex of intestinal and extraintestinal symptoms caused by poor absorption of nutrients in the small intestine.
There are congenital, primary and secondary malabsorption disorders.
Congenital malabsorption disorders have been studied in some detail. Congenital malabsorption malformations are characterized by isolated defects in the transport of individual amino acids, monosaccharides and fatty acids. Congenital malabsorption of minerals and vitamins is very rare.
Primary malabsorption disorders include genetically determined diseases that are caused by substances that have a toxic effect on the mucous membrane (gluten enteropathy, soy enteropathy).
Secondary malabsorption disorders are associated with diseases of the small intestine or other internal organs and are much more common than the previous ones.
Etiology and pathogenesis
The direct cause of the disorder in the absorption of food ingredients may be the reduced activity of digestion enzymes and transport carriers of the final products of digestion through the intestinal wall. Another reason for M. s. is an insufficient supply of enzymes to the intestines with digestive juices due to blockage of the ducts of the glands of the mucous membrane of the small intestine with a viscous secretion, as is observed, for example, in cystic fibrosis. What matters is the lack of formation of enzymes that break down, for example, proteins, which leads to a deficiency of amino acids and protein starvation of the body.
Inactivation of cleavage enzymes and transport carriers also causes the development of M. s. Thus, some antibiotics (chlortetracycline, neomycin) can suppress lipid breakdown processes and increase steatorrhea (see).
When there is an excess of calcium and magnesium salts in food, fat absorption is impaired. In the emergence of M. s. Morphological changes in the small intestine and impaired peristalsis of the gastrointestinal tract are important. tract.
Pathogenetic mechanisms of M. s. diverse. With a deficiency of pancreatic enzymes, the cavity, or pancreatic, phase of digestion suffers; with a deficiency of intestinal enzymes (disaccharidases, peptidases, etc.), the surface, or membrane, phase of digestion is disrupted (see). Intestinal dysbiosis causes changes in the structure of bile cells, hepatobiliary diseases change their metabolism and are accompanied by cholestasis - all this contributes to the disruption of hydrolysis and transport of lipids (biliary phase). In various diseases and lesions of the small intestine, especially in the case of mucosal atrophy, the structures responsible for absorption processes (Cellular phase) are affected to varying degrees. In this case, the absorption epithelium transforms into glandular epithelium, and the diameter of the burrows on the surface of the mucous membrane through which absorption occurs decreases. A number of biochemical defects may occur: the number of transport carriers decreases, their structure changes, as a result of which their ability to interact with transported substances decreases; energy processes that ensure membrane transport are disrupted, etc. As a result of changes in the endocrine functions of the cells of the intestinal wall, the hormonal regulation of digestive and transport processes suffers. In case of disturbances in intestinal lymph flow and mesenteric circulation, further transport of absorbed substances (outflow phase) worsens. When the passage of food masses through the small intestine accelerates, due to motor disorders, the time of contact of chyme with the absorptive surface of the intestine is reduced.
Causes of malabsorption syndrome
The causes of the disease can be very different, but as a rule they are all divided into:
- Congenital and acquired.
- Functional and organic.
- Enzymatic.
- Secondary.
With a group of congenital pathologies, the underdevelopment of the organ or its complete absence most often comes to the fore. This is usually associated with the small intestine.
Besides:
The organ itself may be fully developed, but its mucous membrane may have defects due to which the absorption function will be impaired.
Such lesions can be caused by wall burns, bacterial, viral and fungal damage to the gastrointestinal tract, dietary errors, and radioactive damage.
Another important reason is the failure of the enzymatic apparatus. The intestine itself does not have any damage, but there are no enzymes that should be involved in the processes of food breakdown and digestion. therefore absorption will also be impaired.
Secondary forms occur when an organ is removed, affected by malignant tumors, various forms of colitis, and abdominal injuries.
Classification
There are several classifications of M. s. The following classification testifies to the multiplicity of etiological and pathogenetic factors underlying the occurrence of MS. 1. Primary M. s. (hereditarily determined): intolerance to disaccharides (lactose, sucrose, isomaltose, trehalose) - disaccharidase deficiency; peptidase deficiency (celiac disease); enterokinase deficiency; intolerance to monosaccharides (glucose, galactose, fructose); impaired absorption of amino acids (Hartnup disease, Cystinuria, tryptophan malabsorption, methionine malabsorption); impaired absorption of vitamins - cyanocobalamin (B12), folic acid. 2. Secondary M. s. (acquired): gastrogenic, observed after gastrectomy, with gastritis, stomach cancer; pancreatogenic, caused by various diseases of the pancreas (pancreatitis, cystic fibrosis, cancer, tumors of the islet apparatus, etc.); hepatogenic, observed in acute and chronic liver diseases, intra- and extrahepatic cholestasis; enterogenous, caused by various intestinal diseases (enterocolitis, celiac disease, Crohn's disease, diverticulitis, blind loop syndrome, infectious, parasitic, vascular intestinal diseases), as well as postoperative (resection of the small intestine); endocrine, observed in diabetes mellitus, hyper- and hypothyroidism; so-called Iatrogenic, caused by long-term use of antibiotics, laxatives, cytostatics and other drugs, as well as radiation therapy.
There are other classifications, for example, according to Polonovsky (C. Polonovski, J. Polonovski), the cut is based on the division of M. s. according to the type of its origin (impaired absorption of gastric and intestinal origin, due to bile deficiency, due to pathology of the pancreas).
With primary M. s. Most often, there is a selective deficiency of enzymes or transport carriers and, as a result, the absorption of one food substance or several substances similar in structure suffers.
With secondary M. s. Usually there is a deficiency of many enzymes and transporters, various mechanisms of malabsorption are realized, which leads to impaired absorption of a number of nutrients. Of the primary malabsorption disorders in adults, hl occurs. arr. intolerance to disaccharides (disaccharidase deficiency), mainly lactose, other forms of primary M. s. quite rare, most of them are observed in children. Secondary M. s., especially in an erased form, is relatively often noted in the clinic of gastroenterological diseases of adults.
Forecast
In mild cases, correction can be carried out only with the help of diet. In other cases, the prognosis will directly depend on the course of the disease, primary pathologies and their severity, and the lack of useful components in the body. If you eliminate the primary factor that causes the syndrome, then in the future you will have to correct the patient’s condition, and eliminating the consequences will take a lot of time. If you ignore malabsorption syndrome, it will lead to the development of severe complications and even death.
Malabsorption is a digestive disorder in which disruption of the functioning of the intestine (its small part) leads to problems digesting food and absorbing nutrients. This syndrome causes severe complications, because Metabolism in the body is disrupted, hypovitaminosis, anemia and other problems develop. To diagnose this syndrome, laboratory and instrumental studies are carried out. Treatment should not only cope with the symptoms, but also eliminate the factors that provoked this disease. In addition, therapy should help eliminate dysbiosis, electrolyte, protein, microelement and vitamin deficiencies.
Intestinal dysbiosis Irritable bowel syndrome Intestinal colitis Crohn's disease Intestinal cancer Pancreatitis
Clinical picture
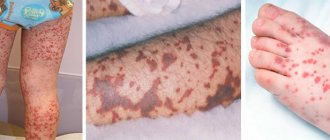
One of the most important wedge, symptoms of M. s. in children it is chronic, diarrhea, and a unique indicator of insufficient absorption is steatorrhea - increased excretion of lipids in feces. The child stops gaining weight, malnutrition develops, and then exhaustion, and growth retardation (hypostature) is observed. Depending on the duration and nature of the process, changes in other organs and systems increase: the skin becomes dry, with a pellagroid coloration; glossitis is pronounced, the tongue is red without papillae; swelling appears due to disturbances in protein and water-electrolyte metabolism; hypochromic anemia, hypokalemia, hyponatremia, hypocalcemia are noted. In some forms of M. s. changes in the urine are observed, for example, with milk intolerance associated with lactose deficiency; in some cases, lactosuria is noted in the urine (see). There may be seizures, osteoporosis or osteomalacia due to calcium deficiency in the body; bloating, intestinal colic due to hypokalemia and increased fermentation processes in the intestines. However, M. s. can proceed without any sharp disturbances from the gastrointestinal tract. tract.
In adults, wedge, picture of M. s. largely due to the nature of the underlying disease. The intensity of intestinal symptoms (stool upset, rumbling, etc.) depends on the degree of intestinal damage, on the involvement of the colon in the patol process, often there are no intestinal symptoms at all. General manifestations predominate, indicating violations of the basic metabolic processes and functions of a number of organs and systems, which is associated with insufficient supply of nutrients to organs and tissues.
Patients complain of increased fatigue, decreased performance, weakness, decreased appetite, weight loss, sometimes exhaustion up to cachexia (see). They experience dry skin, hair loss, and increased brittleness of nails. There may be diarrhea, steatorrhea, creatorrhea. In the blood - hypoproteinemia, dysproteinemia, changes in the composition of blood amino acids, in the urine - hyperaminoaciduria (see Aminoaciduria). The concentration of cholesterol, total lipids and their fractions in the blood serum decreases. Wedges and signs of thiamine deficiency (paresthesia in the limbs, pain in the legs, sleep disorders), riboflavin (cheilitis, angular stomatitis), nicotinic acid (glossitis, pellagroid skin changes), ascorbic acid (bleeding gums) and others are often observed vitamins (see Vitamin deficiency). A number of wedges, symptoms are caused by impaired electrolyte metabolism: hyponatremia (arterial hypotension, tachycardia, dry skin and tongue, thirst), hypokalemia (muscle weakness, muscle pain, weakened tendon reflexes, decreased intestinal motility, extrasystole, etc.), hypocalcemia (numbness of lips and fingers, increased neuromuscular excitability, osteoporosis), manganese deficiency (decreased sexual function). In severe cases, osteomalacia with bone fractures and tetany may occur. Iron deficiency and B12-folate deficiency anemia often occur. In the oral cavity there are atrophic processes, desquamative changes in the tongue, and sometimes periodontopathy. The skin becomes atrophic, dry, folded, acquires a dirty gray color, and pigmentation appears. Cracks appear around the mouth, eyes, and anus; in severe cases, the disease is complicated by eczema and neurodermatitis. Changes in the endocrine system are noted (hypocortisolism, sexual function disorders, etc.); in severe cases, pluriglandular insufficiency syndrome may develop with damage to the pituitary gland, adrenal glands, gonads, and thyroid gland (see Polyglandular insufficiency). Neurotic disorders and hypochondriacal conditions are often observed.
Klin, painting by M. s. to a certain extent depends on the localization patol. process in the small intestine. For example, when its proximal parts are predominantly affected, the absorption of calcium, iron, folic acid, and B vitamins is affected. When the middle parts are affected, the absorption of fatty acids and amino acids is impaired. Absorption of monosaccharides is impaired when the proximal and middle parts of the intestine are affected. When the distal parts of the small intestine are affected, there is insufficient absorption of vitamin B12 and bile cells, therefore, in the case of resection of the ileum, in some forms of Crohn's disease, the enterohepatic circulation of bile cells is disrupted.
With M., especially when the distal ileum is affected, the excretion of oxalates in the urine often increases - enteral oxaluria, which can lead to the formation of oxalate stones.
Severity
Depending on the severity of the disease, the following stages of the disease are distinguished:
- The first degree of severity of the disease. It is considered to be the mildest, at this stage there is a decrease in the patient’s weight, a decrease in the overall level of his performance, an increased feeling of weakness and the appearance of signs of general vitamin deficiency. The patient may lose up to 10 kilograms in weight.
- Second degree of severity of the disease. In this case, there is a noticeable decrease in the weight of the entire body; in approximately half of all cases that occurred, the patient’s body weight decreased by more than 10 kilograms. At the same time, symptoms of vitamin deficiency were clearly manifested, and calcium deficiency was noted in the body. The body also lacks potassium, anemia develops, and the activity of the sex glands decreases.
- Third degree of severity. In the vast majority of cases, at this stage of the disease, the body weight of patients decreases by more than 10-15 kilograms. In addition, the condition is often accompanied by pronounced symptoms of multivitamin deficiency, lack of electrolytes in the body, seizures and pronounced signs of osteoporosis. In addition, anemia gradually develops, patients often begin to complain of general weakness, malaise, they develop swelling in various areas of the body and the functioning of the endocrine gland is disrupted.
Treatment in each case is selected depending on the specific severity of the disease and its symptoms.
Diagnosis
The diagnosis of malabsorption syndrome should be made as early as possible in order to avoid worsening metabolic changes and disruption of various organs and systems.
V. A. Tabolin, E. I. Shcherbatova, T. I. Korneva, V. P. Lebedev, E. K. Kurgasheva (1973) proposed a multi-stage system for clinical and biochemical diagnosis of intestinal malabsorption syndromes in children. The research begins with an assessment of anamnestic data and genealogical analysis (see Genealogical method). At the same time, pay attention to the presence of diseases in relatives. tract (gastritis, peptic ulcer, cholecystitis, enterocolitis, pancreatitis), respiratory system (chronic, bronchitis), metabolic disorders (diabetes mellitus, hyperthyroidism). Along with genealogical analysis, screening tests are envisaged, such as tests for various sugars in feces and urine; scatological examination, determination of stool pH, reaction of stool filtrate with trichloroacetic acid, boiling test. The following tests are used: Benedict's test for sugars, Welk's test for lactose and maltose, Helman's test for sucrose, determination of carbohydrate content in feces using Clinitest tablets using the Anderson method. These tests allow us to identify changes characteristic of individual syndromes.
If celiac disease is suspected (see), the greatest value is the study of the content of total protein, protein fractions, immunoglobulins, total lipids, cholesterol and phosphorus, potassium and sodium in the blood serum, rentgenol. research went.-kish. tract with a suspension of barium sulfate, radiography of long bones, as well as assessment of the effectiveness of the ongoing gluten-free elimination diet - exclusion from the diet of products from rye, wheat, barley and oatmeal (see Celiac disease).
To confirm the diagnosis of M. s. in case of cystic fibrosis (see), it is necessary, along with the determination of sodium and chlorine in sweat fluid, nail plates, and testing with DOX, to study the immune status, the functional state of the liver, as well as the proximal parts of the nephron.
In patients with exudative enteropathy (see Exudative enteropathy), muscle fibers are revealed during scatological examination; qualitative reactions indicate the presence of plasma proteins in the stool. With disaccharidase deficiency, a decrease in stool pH to 5.0 or lower is detected; extracellular starch is found in the coprogram; tests for sugar in urine and stool are positive. Of great importance in the diagnosis of disaccharide intolerance are stress tests with mono- and disaccharides (glucose, D-xylose, lactose, sucrose, etc.) followed by blood tests and their chromatographic identification in feces and urine, as well as the study of daily urinary excretion of carbohydrates and proteins.
If Hartnup's disease is suspected (see Hartnup's disease), along with the characteristic wedge symptoms, the determination of the content of indican, amino acids proline and argine in the urine is of great importance for the diagnosis. Positive tests of verification studies make it possible to conduct more in-depth studies using quantitative analytical methods: blood, daily urine, feces are examined; using an x-ray film test and a test with iodolipol, the activity of trypsin and lipase is assessed; identification of proteins in blood serum and feces is carried out. A study of the daily excretion of carbohydrates in urine reveals melituria (see) in the intestinal form of cystic fibrosis, disaccharidase deficiency, glucose and galactose intolerance. Identification of proteins in blood serum and feces using immunoelectrophoresis (see) makes it possible to diagnose exudative enteropathy. After conducting clinical biochem. By comparing the results obtained, the presumptive diagnosis is confirmed by targeted clinical, radiological and gastroduodenoscopic studies, which are carried out taking into account the data obtained earlier.
All of the listed methods are used in practice to establish the diagnosis of M. s. in adults. Methods for recognizing disorders of the absorption function of the small intestine - see Intestines.
Complications
Malabsorption syndrome can cause the following complications:
- deficiency of various vitamins;
- anemia;
- menstrual irregularities in women;
- severe weight loss or poor weight gain in children;
- deformation of skeletal bones.
The diagram shows the mechanism of formation of complications in malabsorption syndrome
Treatment
In case of primary (hereditarily caused) syndrome of intestinal malabsorption, an important component of complex therapy is treatment. nutrition, which provides for the limitation or exclusion of foods that lead to the development of patol, symptoms. Thus, in the treatment of celiac disease, the main thing is to use a gluten-free diet. A high-calorie diet with sufficient protein, vegetables, and fruits is prescribed; products made from rye, wheat, and oats are completely excluded.
In case of intolerance to disaccharides and monosaccharides, a diet with restrictions is necessary, and in some cases with the exclusion of those sugars that the patient cannot tolerate.
Treatment of lactose intolerance in infants is a difficult task, since in severe forms of deficiency it is necessary to exclude milk from the diet. In these cases, lactose-free milk formulas (galantamine, soyaval) are used. If there is a lack of sucrose, the child should not be transferred to mixed and artificial feeding early. Nutrition of children with intestinal and mixed forms of cystic fibrosis with a predominance of disorders from the gastrointestinal tract. tract, is based on compliance with the standards of products and menus accepted under normal conditions, but with a high content of proteins and carbohydrates, some limitation of fats, and a sufficient content of vitamins and mineral salts.
In case of intolerance to sucrose and isomaltose, sucrose is excluded and starch is limited; in case of intolerance to glucose and galactose, these monosaccharides are sharply limited, fructose is prescribed in increased quantities; in case of celiac enteropathy and other forms of severe enterocolitis, a gluten-free diet is recommended. In case of severe malabsorption of fats (for example, with cystic fibrosis), it is recommended to limit regular fats and prescribe triglycerides containing fatty acids obtained from coconut oil, which are easily hydrolyzed and absorbed in the intestines. In patients with severe forms of M. s. the so-called has a good therapeutic effect. nutritional diet, which is a mixture of amino acids, dextrin, trace elements, vitamins with the addition of small amounts of fat. This diet does not contain lactose, whole protein, is extremely low in waste and fat, and does not contain allergens.
Therapy for secondary (acquired) intestinal malabsorption syndrome involves treating the underlying disease. In severe cases M. s. Parenteral nutrition courses (glucose, protein hydrolysates, basic electrolytes, vitamins) are very effective. With M. s. due to intestinal dysbiosis, short courses of broad-spectrum antibiotics or eubiotics (8-hydroxyquinoline derivatives, Bactrim, etc.) are indicated; biol drugs (colibacterin, bificol, bifidumbacterin, etc.) are also recommended.
An essential role among to lay down. measures are played by means of replacement therapy. Preparations of pancreatic enzymes (Pancreatin, Panzinorm Forte, etc.), Abomin and a number of other enzyme preparations are prescribed; Only large dosages of these drugs are effective. The administration of enzyme preparations together with antacids, which significantly inhibit gastric secretion, helps to enhance the therapeutic effect of enzyme preparations for M. s. due to pancreatic insufficiency. Vitamins (A, D, K, C, folic acid, complex B, B12), calcium, magnesium, iron, cobalt are prescribed in pharmacodynamic doses. The administration of protein preparations (plasma, protein hydrolysates, protein, etc.) is indicated. With M. s. Cholestyramine is recommended due to dysfunction of the ileum (after its resection, in Crohn's disease, etc.), lignin (polyphepan) can be used for the same purpose, adsorbing unabsorbed bile cells and promoting their excretion in feces.
In cases of secondary M. s., caused by hl. arr. insufficient activity of membrane digestion enzymes, Difril (Corontin) in sufficient doses (at least 180 mg per day), as well as anabolic steroids (Nerobol, etc.), which stimulate the processes of membrane hydrolysis in the small intestine, are indicated. The phosphodiesterase inhibitor aminophylline and the inducer of lysosomal enzymes phenobarbital also increase the activity of membrane digestive enzymes. Some adrenomimetic drugs stimulate the absorption of monosaccharides in the small intestine - ephedrine, L-dopa, beta-blocker propranolol (obzidan, anaprilin), deoxycorticosterone acetate, aminophylline. The kinin inhibitor prodectin (parmidine), anticholinergic (atropine) and ganglion-blocking (benzohexonium) drugs have a normalizing effect on the absorption of monosaccharides - and at low initial rates they stimulate it, at high levels they inhibit it. For diseases where M. s. is secondary, when malabsorption is not associated with a deficiency of digestive enzymes or transport carriers, correction of intestinal absorption processes with the help of medications can be effective.
What happens in the body with SMA
Normally, food digestion occurs in 3 phases:
- breakdown of proteins, fats and carbohydrates with the help of enzymes in the intestinal lumen;
- absorption of the final products of food digestion with the help of microvilli of enterocytes (cells of the intestinal mucosa);
- transport of nutrients through lymphatic vessels.
If any of these phases are disrupted, the child experiences malabsorption.
Taking into account the localization of the digestive disorder, the following forms of SMA are distinguished:
- cavitary: congenital digestive disorders in the intestinal lumen;
- enterocellular: associated with disruption of membrane digestion or nutrient transport;
- postcellular: occurring in older children, associated with increased release of blood plasma proteins into the intestinal lumen.
Unabsorbed fats are released along with fat-soluble vitamins, and hypovitaminosis develops. Bile salts are also poorly absorbed (microflora causes a limitation of their absorption). They cause irritation of the large intestine, which is the cause of diarrhea in a child.
When the digestion of carbohydrates is impaired, they are broken down by microflora enzymes into carbon dioxide, methane, hydrogen and fatty acids, which cause diarrhea. The resulting gases cause bloating (flatulence).
The digestion and assimilation of proteins requires the enzyme enterokinase, secreted by the microvilli of enterocytes. With a deficiency of this enzyme, protein deficiency develops in the body.
SMA in a child at an early age leads to severe metabolic disorders and disruption of not only physical but also mental development. Malabsorption is especially dangerous for infants, as it can quickly lead to depletion of the body and even death.
Prognosis and Prevention
Forecast for primary M. s. depends on the timeliness of the diagnosis and the correctness of the treatment; in case of secondary MS, it depends on the underlying disease and the effectiveness of the treatment.
Prevention of secondary M. s. consists of treating the underlying disease.
Bibliography:
Badalyan L. O., Tabolin V. A. and Veltishchev Yu. E. Hereditary diseases in children, p. 231, M., 1971; Vasilenko V. X. and Vinogradova M. A. About the problem of insufficient absorption of nutrients and the classification of its form, Klin, med., t. 45, No. 2, p. 9, 1967; Veltishchev Yu. E. et al. About intolerance to disaccharides in childhood, Vopr. ocher mat. and children, vol. 14, no. 12, p. 3, 1969, bibliogr.; G at b e r g r and c A. Ya. and L and Nevsky Yu. V. Diseases of the small intestine, M., 1975, bibliogr.; Complex therapy for diseases of the digestive system, ed. H. T. Larchenko and A. R. Zlatkina, M., 1977; Loginov A. S. et al. Treatment of patients with chronic diseases of the small intestine, Sov. med., No. 2, p. 63, 1979; Tabolin V. A. et al. Issues of diagnosis and treatment of malabsorption syndromes in children, Pediatrics, No. 3, p. 3, 1974; Physiology of absorption, ed. A. M. Ugoleva et al., L., 1977; F r about l-kiye A. V. Chronic enterocolitis, L., 1975, bibliogr.; Ament M. E. Malabsorption syndromes in infancy and childhood, J. Pediat., v. 81, p. 685, 1972; Bond JH a. L evitt MD Quantitative measurement of lactose absorption, Gastroenterology, v. 70, p. 1058, 1976; Gastrointestinal disease, ed. by M. H. Slei-senger a. J. S. Fordtran, p. 259, Philadelphia, 1973, bibliogr.; L osowsky MS, Walker BE a. K e 1 1 eher J. Malabsorption in clinical practice, Edinburgh, 1974, bibliogr.; Regan PT Konservative Therapie der Malabsorption, Leber Magen Darm, Bd 7, S. 201, 1977, Bibliogr.; Schreier K. Maldigestions-und Ma-labsorptionsyndrome, in the book: Klin. Gastroenterol., hrsg. v. L. Demling, Bd 1, S. 302, Stuttgart, 1973.
A. V. Frolkis; V. A. Tabolin (ped.).
Diagnostics
Diagnosis of malabsorption syndrome is quite simple, but labor-intensive. To do this, you need to undergo a series of not only laboratory tests, but also instrumental ones:
- history taking and symptom assessment;
- initial examination. With the help of palpation, the doctor has the opportunity to identify tension in the anterior abdominal wall, as well as areas on the abdomen in which the patient feels pain;
- blood analysis. With malabsorption, there is a decrease in hemoglobin, as well as red blood cells;
- blood biochemistry;
- coprogram. Dietary fiber, particles of undigested food, fats, etc. can be found in excrement;
- Ultrasound;
- esophagogastroduodenoscopy;
- colonoscopy;
- CT or MRI.
What needs to be examined?
- Small intestine (small intestine)
- Colon (large intestine)
What tests are needed first?
- General blood analysis
- Stool analysis
The diagnosis should be made only after a comprehensive examination of the patient.