Plague disease is caused by the zoonotic bacterium Yersinia pestis, which is usually found in the bodies of small mammals and in the fleas that live on them. The infection is transmitted between animals by fleas. Human infection can occur as a result of:
- bite of an infected flea - a carrier of the disease;
- unprotected contact with infected body fluids or contaminated materials;
- inhalation of infected small particles/fine droplets exhaled by a patient with pneumonic plague (airborne).
In humans, plague, especially its septic (as a result of bacteria entering the bloodstream) and pneumonic forms, without treatment can be a very serious disease with a fatality rate of 30-100%. Without early treatment, the pulmonary form always leads to death. It is particularly contagious and can cause severe epidemics, transmitted from person to person by airborne droplets.
In 2010-2015 There were 3,248 cases of plague reported worldwide, including 584 deaths.
In the past, plague has caused large-scale pandemics with high mortality rates. In the 14th century, the plague was known as the Black Death and killed an estimated 50 million people in Europe. Today, plague is easily treated with antibiotics, and preventing infection is not particularly difficult if standard precautions are followed.
Signs and symptoms
A person infected with the plague usually develops an acute febrile state after an incubation period of 1 to 7 days. Typical symptoms include sudden fever, chills, headache and body aches, as well as weakness, nausea and vomiting.
Depending on the route of infection, there are two main forms of plague infection: bubonic and pneumonic. All forms of plague are treatable if detected early enough.
- Bubonic plague
is the most common form of plague in the world and is caused by the bite of an infected flea. The causative agent of plague, the bacterium Yersinia pestis, enters the human body at the site of the bite and moves through the lymphatic system to the nearest lymph node, where it begins to multiply. The lymph node becomes inflamed, swells and creates pain; such lymph nodes are called “buboes”. In later stages of infection, swollen lymph nodes may turn into open, purulent sores. Person-to-person transmission of bubonic plague is rare. If bubonic plague continues to develop, the infection may spread to the lungs, resulting in a more severe form of plague called pneumonic plague. - Pneumonic plague
is the most virulent form of this disease. The incubation period can be extremely short, as little as 24 hours. Any person with pneumonic plague can transmit the infection to others through airborne droplets. Without early diagnosis and treatment, pneumonic plague is fatal. However, if detected and treated early (within 24 hours of symptom onset), a significant proportion of patients are cured of the disease.
What diseases can it be associated with?
Complications of plague depend on the clinical form. With bubonic plague, a secondary infection may occur with the development of adenophlegmon, as well as the development of secondary septicemia. The course of pneumonic plague is complicated by hemorrhagic pulmonary edema, acute respiratory failure and infectious-toxic shock. With septic plague, ITS, acute heart failure (AHF), meningitis, and bleeding can develop.
In the absence of adequate treatment, the mortality rate for bubonic plague reaches 70%, and with treatment - 10-20%. The mortality rate for pneumonic plague in the case of treatment is 30-50%, and in the absence of it - 100%. The mortality rate for septicemic plague in the absence of treatment is also 100%.
Where does the plague occur?
As an animal disease, plague is found everywhere, with the exception of Oceania. The risk of human plague occurs when a single population of people lives in an area where there is a natural source of plague (i.e., bacteria, animal reservoirs and vectors).
- Map of the distribution of natural plague foci in the world as of March 2021, pdf, 48Kb - in English pdf, 48kb
Plague epidemics have occurred in Africa, Asia, and South America, but since the 1990s, most human plague cases have occurred in Africa. The three most endemic countries are: Madagascar, Democratic Republic of the Congo and Peru. In Madagascar, cases of bubonic plague are reported almost every year during the epidemic season (September-April).
Diagnostics
Considering that plague is a rather rare phenomenon, the timeliness of diagnosis largely depends on the vigilance of the doctor and the consciousness of the patient. Therefore, those people who had a risk of becoming infected (for example, tourists visiting India, China, Madagascar, Mozambique, Kenya and other countries with a high probability of infection - especially if there were flea bites; people who took part in the slaughter of a camel or the processing of its skin) At the first symptoms, you should consult a doctor and report the possibility of infection.
The doctor will be sure to ask any patient with signs of plague about such travel and contacts. This is called epidemiological diagnosis .
The next stage is clinical diagnosis . The doctor will examine the patient and ask about the onset of symptoms and their intensity.
The third stage is laboratory research aimed at identifying bacteria, determining the form of the disease and differentiating the plague from other diseases with similar symptoms.
The reliability of diagnosis deserves greater confidence if the doctor cooperates with a laboratory that employs experienced employees. Since the plague has a low prevalence, there are not many experienced specialists in it.
First, the doctor will take the necessary materials for bacteriological examination:
- Blood. It is taken from all patients, regardless of the expected form of the disease. Typically, the material for research is taken from the ulnar vein.
- The contents of the inflamed lymph node - if the bubonic form is suspected. A puncture is performed to collect material for analysis. The puncture is taken with a sterile needle; it is advisable to take an analysis from the center of the lymph node. Since inflamed lymph nodes are very painful at the initial stage of the disease, the procedure is performed under local anesthesia.
- A sputum sample is taken if pneumonic plague is suspected.
- A throat swab is taken if there is no sputum or if the oropharyngeal form is suspected.
- If plague meningitis is suspected, a lumbar puncture is performed to examine the cerebrospinal fluid.
- Discharge from ulcers and puncture of carbuncles if a cutaneous form of the disease is suspected. To do this, first clean the skin around the area with a sterile napkin, remove pus and necrotic mass. Then the ulcer is carefully soaked with a swab.
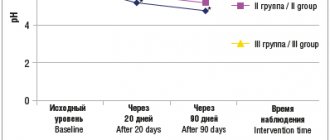
A blood test for plague will show an increase in the number of neutrophils, a decrease in platelet volume, and an increased level of leukocytes and bilirubin. Some of the blood is tested for antibodies to the plague bacillus, and some is used for bacteriological culture. However, culture results usually take at least a day to prepare. Bacteria can be identified by staining with aniline dyes; Gram staining is negative.
PCR testing is considered the fastest. With its help, bacterial DNA is detected in the patient's biological fluids. The research result can be obtained quickly, but this requires a well-equipped laboratory.
In addition to laboratory tests, to confirm the diagnosis, the doctor may prescribe an X-ray examination of the lungs and an ultrasound scan of the lymph nodes.
Since infectious agents are detected in the blood with bubonic plague, as with the septic form of the disease, it is very important to differentiate these forms, since septic requires more urgent and intensive treatment. Therefore, it is important for the doctor to pay attention to changes in the patient’s lymph nodes.
The cutaneous form should be distinguished from anthrax. The latter is characterized by an increase due to the combination of several pustules.
Oropharyngeal plague has no symptoms that distinguish it from ordinary sore throat. Therefore, in areas prone to infection, physicians and patients need to be aware of the importance of timely differential diagnosis.
Treatment
Without treatment, plague can lead to rapid death, so the most important condition for patient survival and prevention of complications is rapid diagnosis and early treatment. With timely diagnosis, plague can be successfully treated with antibacterial drugs and supportive care. Untreated pneumonic plague can be fatal within 18 to 24 hours of symptoms appearing, but common antibiotics for diseases caused by Enterobacteriaceae (Gram-negative rods) can effectively cure the plague if treated early.
Fighting plague outbreaks
- Detection and neutralization of the source of infection:
identification of the most likely source of infection in the area where the case(s) of human disease has been identified, paying special attention to areas where small animal carcasses accumulate. Implement appropriate infection control measures. You should avoid exterminating rodents before exterminating fleas that carry the infection, since fleas will transfer from a dead rodent to a new host and the spread of infection will continue. - Protecting the health of healthcare workers:
informing and training healthcare workers on infection prevention and control measures. Workers who have been in direct contact with persons infected with pneumonic plague should wear personal protective equipment and receive antibiotics as chemoprophylaxis for seven days, or at least for as long as they are exposed to the risk of working with infected patients. - Ensuring correct treatment:
Ensuring that patients receive appropriate antibiotic treatment and that there is an adequate supply of antibiotics. - Isolation of patients with pneumonic plague:
Patients should be isolated to prevent airborne spread of the infection. Providing protective face masks to these patients may reduce the risk of spreading infection. - Surveillance:
identifying and tracking close contacts of pneumonic plague patients and administering chemoprophylaxis to them for 7 days. - Obtaining samples,
which should be collected with care, following all preventive measures and infection control procedures, and then sent to laboratories for testing. - Disinfection:
It is recommended to regularly wash your hands with soap and water or use alcohol-based hand sanitizer gels. To disinfect large areas, you can use a 10 percent solution of household bleach (the solution should be renewed daily). - Observe precautions when burying the dead:
spraying antiseptics on the face/chest of corpses of patients believed to have died from pneumonic plague is inappropriate and not recommended. Cover the area with an antiseptic-impregnated cloth or absorbent material.
City under siege
View of the town hall in Marseille during the great plague of 1720. Michelle Serre. 1721 Musée des Beaux-Arts de Marseille
The plague-ridden city quickly turns into a besieged fortress. But he is besieged not only from the outside, but also from the inside. His enemy is infection. And everyone who is still healthy has a potential enemy - anyone who is already sick. Neighborhoods, streets, houses, people - the city breaks up into many small fortresses fighting for survival. The history of epidemics, during which death sweeps away all conventions, exposes the fragility of social ties.
Sometimes it seems that if you don’t notice the danger, it will pass by. In many cities, when the first cases appeared, residents did not want to believe that the plague had returned. The authorities delayed introducing quarantine and other restrictions, fearing to provoke panic, cut off the city from food supplies and collapse its finances. What if it’s not a plague after all? What if the doctors are mistaken or are deliberately intimidating everyone about the epidemic in order to profit at the expense of their fellow citizens? What if the pestilence passes?
In 1599, when the plague was raging throughout the north of Spain, doctors in Burgos and Valladolid, not wanting to admit the obvious, made evasive diagnoses: “This is not really a plague,” “We are talking about tertiary and double fever, diphtheria, fever, stitches in the side, catarrh, gout and similar diseases... Some patients have buboes, but they are easily cured.” Alas, many of the buboes did not last, and Burgos and Valladolid were devastated. The epidemic is almost always “foreign”. It comes from foreign lands, and maybe even sent from there. In Lorraine in 1627 the plague was called “Hungarian”, and in 1636 - “Swedish”; in Toulouse in 1630 - “Milanese”.
Saint Macarius of Ghent gives Holy Communion during the plague. Jacob Van Ost the Younger. 1673 Musée du Louvre
The pestilence was doubly destructive: it devoured not only the cells of the body, but also the cells of society. When collective prayer services and religious processions could not appease the angry God, religious zeal gave way to disunity. After all, a stranger who prays next to you risks becoming your unwitting killer. Witnesses of the epidemic in Florence (1348), Brunswick (1509), London (1664–1665), Marseilles (1720), as if from a carbon copy, described how parents abandon sick children, children run away from their parents, husbands betray their wives, and wives forget about husbands. During the Milanese plague of 1630, some townspeople went out into the streets, armed with a pistol, so that no one would dare to approach them. The plague swept away the usual way of life and urban order. Almost always during a pestilence, there were rumors that plague inspectors were robbing houses, and gravediggers, in order not to return to the same house twice, threw people into their carts and buried those still alive.
“...The disaster instilled such horror in the hearts of men and women that brother left brother, uncle of nephew, brother’s sister, and often husband’s wife; Moreover, and more incredible: fathers and mothers avoided visiting their children and following them, as if they were not their children. For this reason, men and women who fell ill, and their numbers cannot be counted, had no other help left except the mercy of friends (there were few of them) or the greed of servants attracted by large, out-of-measure salaries; and there were not many of them, and they were men and women of a rude disposition, not accustomed to this kind of care, who did not know how to do anything else but give the sick what they needed, and look after them when they ran out; While serving such service, they often lost their lives along with their earnings.”
Giovanni Boccaccio. "Decameron"
In some cities, priests and doctors, whose mission was to console the desperate and care for the incurable, abandoned churches and hospitals. In others, they stayed to fulfill their duty and died along with the sick and their flock. In Perpignan in 1348, six doctors out of eight died, in Florence - 78 cordillera monks out of 150. In Milan, during the epidemic of 1575, Archbishop Carlo Borromeo remained in the city and consoled the sick in hospitals. His nephew Federico, who also became an archbishop, did the same thing 55 years later. But there were also many church hierarchs who fled from the plague, leaving their parishioners behind.
The proximity of death often led to psychological extremes: the apathy of hopelessness was replaced by unbridled joy, and mourning by revelry. Since the end is on the threshold, you need to have time to enjoy life. Moralists castigated contemporaries who indulged in gambling and debauchery in the midst of the spectacle of death. And in Paris in 1401, the Dukes of Burgundy and Bourbon created the “court of love” (cour amoureuse). It was a kind of club or courtly community, intended for joint feasts and literary exercises in honor of the ladies. His goal was to “pass the time with grace and find new joy in life” during the “difficult time of the plague.”
Sheltered from the Florentine plague in the church of Santa Maria Novella. Miniature by Taddeo Crivelli for “The Decameron” by Giovanni Boccaccio. 1467 Bodleian Lipary, Oxford
It was possible to find a scientific basis for earthly joys. Many doctors of the 16th and 17th centuries argued that apathy and fear greatly increased the risk of infection, and therefore prescribed moderate entertainment, music and pleasant reading as medicine. At times, city authorities even organized public festivals in the midst of the epidemic in order to prevent hopelessness from taking precedence over hope. When the plague subsided, many cities were gripped by wedding fever: people who had lost their families hurried to get married in order to forget about the horror of death. According to some reports, in Cologne, shortly after the plague of 1451, which killed more than 20 thousand people, 4 thousand marriages took place.
“Some believed that a moderate life and abstinence from all excesses greatly help in the fight against evil; having gathered in circles, they lived, separated from others, taking refuge and locking themselves in houses where there were no sick people... they spent time among music and the pleasures that they could provide themselves. Others, carried away by the opposite opinion, argued that drinking and enjoying a lot, wandering around with songs and jokes, satisfying, if possible, every desire, laughing and mocking everything that happens - this is the surest cure for the disease. And as they said, they carried it out to the best of their ability, wandering day and night from one tavern to another, drinking without restraint and measure, most often arranging this in other people’s houses, just so they would hear that there was something there to their taste and taste. pleasure".
Giovanni Boccaccio. "Decameron"
Surveillance and control
Surveillance and control requires surveying of animals and fleas involved in the plague cycle in the region, as well as the development of environmental control programs aimed at understanding the natural zoonotic nature of the infection cycle and limiting the spread of the disease. Active, long-term surveillance of animal foci, accompanied by immediate response measures during outbreaks of disease among animals, can successfully reduce the number of outbreaks of plague among humans.
To effectively and efficiently respond to plague outbreaks, an informed and vigilant health workforce (and local community) is essential to quickly diagnose cases and provide appropriate care to those infected, identify risk factors, conduct ongoing surveillance, control vectors and their hosts, laboratory confirmation of diagnoses and transmission of information on test results to the competent authorities.
WHO response
WHO's goal is to prevent outbreaks of plague by conducting surveillance and helping high-risk countries develop preparedness plans. Because the reservoir of infection in animals may vary by region, influencing the level of risk and conditions of transmission to humans, WHO has developed specific recommendations for the Indian subcontinent, South America and sub-Saharan Africa.
WHO is working with ministries of health to support countries experiencing outbreaks to implement local outbreak control measures.