Paraproctitis or pararectal abscess is an inflammation of the tissues located around the rectum. Among proctological diseases, perirectal abscess occupies one of the leading places in terms of frequency of occurrence.
According to various data, among patients who consult a proctologist, from 20 to 40% have paraproctitis. If you contact a doctor late or if the treatment tactics for this disease are incorrect, complications develop, and the acute process becomes chronic, which worsens the prognosis.
Classification
There are several different classifications of acute paraproctitis. Let's look at each of them.
The first classification is based on the etiology of this pathology:
- Common acute paraproctitis, resulting from constipation and subsequent infection;
- The acute form of anaerobic paraproctitis is diagnosed in the case of an anaerobic infection;
- A specific form of acute paraproctitis;
- Acute paraproctitis of traumatic nature. Occurs as a result of chemical or mechanical damage to tissue.
The following classification is based on the localization of the resulting fistulas or infiltrates:
- Subcutaneous acute paraproctitis. The purulent infiltrate is localized under the skin in the anal area.
- Ishiorectal acute paraproctitis. Occurs in 38-40% of cases.
- Retrorectal acute paraproctitis is called an abscess and occurs in 1.5, less often 2% of patients who apply.
- Submucosal acute paraproctitis. The inflammatory process is localized directly under the mucous layer of the rectum.
- Pelviorectal acute paraproctitis. The lesion is localized in the fatty tissue located above the pelvic diaphragm.
- Necrotizing paraproctitis.
There is a classification of chronic paraproctitis based on the anatomical features of the fistulas formed as a result of the pathological process:
- Complete fistula. The formed formation has both one and several different passages, merging into one with a common hole on the surface of the skin.
- Incomplete fistula. There is no fistula opening on the surface of the skin. The passage opens onto the intestinal mucosa.
- External fistula. The lesion has access to the surface of the skin.
- Internal fistula. Both exits open into the pelvic cavity or intestinal space.
The following classification is based on the direction of the opening of the fistula:
- Side;
- Front;
- Rear.
Depending on the nature of the location of the fistula opening relative to the anal sphincter, several different types of paraproctitis are distinguished:
- Intrasphincteric, i.e. the fistula is localized to the sphincter on the intestinal side and is diagnosed in 30-35% of cases. It is characterized by the presence of a focus of inflammation without branching fistula tracts.
- Extrasphincteric. The opening of the fistula is located outside the sphincter on the outside.
- Transsphincteric. Doctors find fistula fibers directly in the sphincter area. A characteristic feature is the presence of several purulent tracts, complicating treatment. Gradually, scarring of purulent pockets and the formation of new fistula tracts occurs.
Classification of pararectal abscesses
According to the activity of inflammation:
- Acute perirectal abscess - has an acute onset and pronounced symptoms.
- Infiltrative – there is infiltration of surrounding tissues.
- Chronic - fistulas are formed that must be excised surgically.
According to the location of the source of inflammation:
- Subcutaneous abscess
- Submucosal abscess
- Ischiorectal abscess
- Pelvic-rectal abscess
According to the location of the internal opening of the fistula:
- Rear position
- Front location
- Lateral position
According to the depth of tissue damage by the inflammatory process:
- Deep abscess
- Superficial abscess
Causes of the disease
The main culprits of paraproctitis are anaerobic bacteria: E. coli, often in collaboration with staphylococci and streptococci.
The infection enters the tissue surrounding the rectum through the gland ducts (Morgani's crypts) that open into the anal canal or through microdamages in the rectal mucosa.
The hematogenous/lymphogenous route of spread of infection cannot be excluded. The pathogen from chronic foci of infection (caries, sinusitis, chronic tonsillitis) reaches the anal zone through the blood or lymph and multiplies in the peri-rectal tissue.
Factors provoking the development of paraproctitis:
- haemorrhoids,
- nonspecific ulcerative colitis,
- anal and rectal fissures,
- Crohn's disease,
- constipation,
- reduced immunity,
- atherosclerosis of rectal vessels,
- gynecological diseases in women and prostatitis in men,
- diabetes,
- surgery on the rectum.
Complications of paraproctitis
If acute paraproctitis is not cured in time, pus can break through the skin - in this case, a fistula is formed and chronic paraproctitis develops. But more often, pus begins to spread throughout the surrounding tissues, forming extensive phlegmons (foci of purulent tissue melting). In especially severe cases, it can break into the peritoneum, causing peritonitis, or provoke sepsis (blood poisoning).
With long-term chronic paraproctitis, it is possible to replace muscle fibers with scar connective tissue (pectenosis), which disrupts the normal functions of the rectum: with formed stool, it is difficult to empty the intestines, and liquid feces do not hold.
Symptoms
The clinical picture of paraproctitis (see photo) varies significantly depending on the location of the purulent focus. At the onset of the disease, there is a short period of malaise, weakness and headache. There is an increase in temperature above 37.5°C with chills.
With subcutaneous paraproctitis , when the abscess is located near the anus under the skin, the symptoms are the most striking: a painful tumor in the anus, with redness of the skin above it. The pain gradually increases, becoming intensely pulsating, making it difficult to sleep and sit, defecation becomes extremely painful, and softening appears above the tumor. This form of paraproctitis occurs most often.
A submucosal abscess is located under the mucous membrane of the rectum. Symptoms for this type of location are similar to subcutaneous paraproctitis, but pain and skin changes are less pronounced.
In an ischiorectal abscess, the purulent focus is located above the levator ani muscle. Due to the deeper location of the abscess, local symptoms are more vague: dull throbbing pain in the pelvis and rectum, aggravated by defecation. Changes in the skin in the form of redness, swelling, swelling occur later 5-6 days after the onset of pain. The general state of health is poor: the temperature can rise to 38°C, and intoxication is pronounced.
Pelviorectal abscess is the most severe . This is a rare form of acute paraproctitis, when the purulent focus is located above the muscles that form the pelvic floor and is separated from the abdominal cavity by a thin layer of peritoneum. At the onset of the disease, severe fever, chills, and joint pain predominate. Local symptoms: pain in the pelvis and lower abdomen. After 10-12 days, the pain intensifies, stool and urine retention appears.
Necrotizing paraproctitis is classified into a separate group . This form of paraproctitis is characterized by the rapid spread of infection, is accompanied by extensive necrosis of soft tissues and requires their excision, after which large skin defects remain that require skin grafting.
Chronic paraproctitis manifests itself as purulent fistulas.
The mouths of the fistula tracts can be located near the anus of the rectum or at a distance from it on the buttocks. The pain is usually not pronounced. Pus mixed with feces is often released from the mouth of the fistula. During the development of chronic paraproctitis, the fistula opening may close, pus retention occurs, abscesses develop, new tissue defects appear, pus breaks through and flows into the rectum and out, necrotization and other tissue changes that significantly complicate fistulas. Thus, complex fistula systems arise with branches of the fistula tract, cavity depots and many openings.
Paraproctitis
Paraproctitis is a purulent inflammation of the tissues surrounding the rectum (peri-rectal tissue), caused by the penetration of an infectious process from the lumen of the rectum. Paraproctitis can be both acute and chronic. In acute paraproctitis, a purulent abscess most often forms, which is characterized by severe pain in the anus and perineum. Disturbances in bowel movements, fever, and chills may also occur.
Chronic paraproctitis often develops as a consequence of neglected (with untimely or insufficient treatment) acute paraproctitis or other infectious processes in the rectum and anal area. In the chronic course of the disease, perirectal fistulas often form. Such fistulas are long-term pathological channels between the rectum and the skin of the perianal area or nearby internal organs. It is worth noting that chronic paraproctitis is a fairly common disease, accounting for about 20-30% of all diseases of the rectum. At the same time, men, mostly young and middle-aged, suffer from paraproctitis more often. However, paraproctitis can develop in a person of any gender and age.
Why does paraproctitis occur?
Paraproctitis is an inflammatory disease of an infectious nature, which occurs when an infection penetrates into the peri-rectal tissue, which normally does not contain any microorganisms. In most cases, the infection is caused by bacteria that make up the normal intestinal microflora (Escherichia coli, staphylococci, Proteus, streptococci, enterococci and some others). Penetration of these bacteria through the wall of the rectum is possible in the presence of the smallest cracks in the rectum, as well as in cases of trauma to the rectal mucosa caused by any factors. In addition, predisposing factors for the development of acute paraproctitis are the presence of hemorrhoids, persistent bowel problems (both constipation and diarrhea), acute prostatitis (inflammation of the prostate gland) and the presence of any previous operations involving the anorectal area or rectum.
Thus, the list of provoking factors for acute paraproctitis is quite wide and includes:
- Cracks and injuries to the rectum (for example, due to constipation)
- Acute infections of other organs and tissues (for example, purulent tonsillitis)
- Bowel problems (diarrhea and constipation)
- Systemic diseases involving blood vessels (diabetes mellitus, atherosclerosis)
- Chronic diseases of the perianal space, anal canal or rectum (for example, hemorrhoids)
- Previous rectal surgery
- Sexually transmitted diseases (for example, gonorrhea, which develops during unprotected anal sex)
- Weakening of local and general immunity
Symptoms and signs of paraproctitis
As a rule, the first symptom of acute paraproctitis is pain in the rectum and perianal area, which can significantly intensify during bowel movements. The pain can have varying degrees of intensity and spread to different parts of the body surrounding the pelvis. In addition, over time, the pain may become worse and occur with movement or even when urinating. Sometimes the first symptom of paraproctitis can be a high temperature, but usually fever develops after the formation of an abscess and the appearance of pain. In addition, the general intoxication syndrome that occurs as a result of the infectious-inflammatory process will include:
- Chills and fever (usually mild fever)
- Weakness, weakness and increased fatigue
- Headache, muscle pain
- Decreased or lack of appetite
Local signs of acute paraproctitis include redness, swelling and severe pain when touching the perianal area. When pathological canals (fistulas) form between the inside of the rectum and the skin, the external opening of this canal will be visible. In addition, purulent, bloody or even fecal discharge may be observed from the fistulas. Most often, the discharge is not abundant, but it can be painful and lead to additional irritation and inflammation in the anogenital area.
Chronic paraproctitis, unlike acute paraproctitis, is characterized by less pronounced symptoms of intoxication and a long, wave-like course, in which periods of exacerbation and periods of remission alternate. When a period of exacerbation of chronic paraproctitis occurs, the symptoms resemble those in the acute form of the disease. An increase in temperature, redness and severe pain in the anogenital area and other symptoms described above are observed. During remission, the intensity of these symptoms may decrease significantly or be completely absent, however, when the body is exposed to predisposing or trigger factors, a repeated exacerbation will be observed. Such provoking factors include, for example, a decrease in the general protective properties of the body and trauma to the rectum. With chronic paraproctitis, in almost all cases there will be a rectal fistula. During remission, the visible size of the fistula (for example, the size of its external opening) will decrease, but mucus or even feces may still be released.
What types of rectal fistulas are there?
Rectal fistulas according to their structure are divided into complete, incomplete and internal. Complete fistulas always have two formed openings: an internal one, opening directly into the rectum, and an external one, connecting the rectum to the perianal area. In incomplete fistulas, there is no external opening or has not yet formed, and in internal fistulas, both openings go directly into the lumen of the rectum. To determine the exact structure of the fistula canal, it is necessary to conduct special X-ray studies using a contrast agent (fistulography). Knowledge of the exact anatomy of the fistula tract greatly helps in the surgical treatment of paraproctitis, facilitating the operation and leading to better results.
In addition to permanent aesthetic defects and discomfort, fistulas can also become extremely easily infected and inflamed, leading to another exacerbation of the disease. It must also be remembered that the presence of constant inflammation is a factor predisposing to cancer transformation and the occurrence of malignant neoplasms. It is precisely because of the described factors that acute and chronic paraproctitis must be treated in a timely manner.
What forms and types is paraproctitis divided into?
In addition to dividing according to the course of the disease (acute and chronic form), paraproctitis can also be divided according to the location of the abscess:
- Subcutaneous paraproctitis, in which the abscess is located directly under the skin of the perianal area. With this location of the abscess, it can often be palpated by hand, which allows the doctor to quickly suggest a diagnosis and prescribe treatment.
- Submucosal paraproctitis, in which the abscess is located inside under the mucous membrane of the rectum. In these cases, it is more difficult to diagnose paraproctitis during examination, but sometimes you can palpate the abscess during a rectal digital examination.
- Deep forms of paraproctitis, in which:
The abscess is located next to the levator ani muscle - ischiorectal paraproctitis;
The abscess is located deep in the pelvis - pelviorectal paraproctitis;
The abscess is located deep behind the rectum - rectal paraproctitis.
If the abscess is deep, it cannot be palpated and for diagnosis it is necessary to resort to hardware methods: ultrasound or computed tomography of the pelvic organs.
Diagnosis of paraproctitis
When you see a doctor, you will first be asked about your complaints, including complaints of pain in the perianal area, their intensity and how long ago they appeared. The doctor will also ask you about any possible factors that increase or decrease the pain, previous surgeries, any trauma to the rectum, your sex life, and any chronic medical conditions you have. If you have or have ever had a chronic disease, especially one involving the gastrointestinal tract (such as ulcerative colitis), you should tell your doctor.
After collecting an anamnesis, you will be examined, with the help of which the doctor will be able to see signs of paraproctitis and differentiate it from other possible conditions. In addition, an examination sometimes allows one to immediately assume or make a correct diagnosis. For example, with subcutaneous paraproctitis, when the abscess is located directly under the skin of the perianal area, as described earlier, it can be palpated. However, other forms of the disease (submucosal and deep forms) often cannot be recognized during external examination, and this requires specific procedures, including ultrasound or computed tomography of the pelvic organs. These studies also make it possible to assess the exact location and size of the abscess, the presence of fistula ducts, or the development of any complications. In the presence of a fistula canal, a special x-ray method is also performed to study the canal cavity using a contrast agent - fistulography. It allows you to determine the direction, shape and configuration of the canal, assess its length and relationship with nearby organs, and also find out where the internal opening of the fistula exits. This information is necessary before performing a surgical operation to excise the fistula and restore the normal anatomy of the perirectal region. Knowing this data, the surgeon will be able to purposefully and quickly perform the operation, improving the outcome, reducing the recovery time after surgery and reducing the likelihood of complications.
The doctor will also prescribe mandatory laboratory blood tests to assess the inflammatory process, including a complete blood count and ESR. With acute paraproctitis and the onset of exacerbation of chronic paraproctitis, you can often see an increase in the content of white blood cells (leukocytes) and an increase in the erythrocyte sedimentation rate (ESR), as well as an increase in the amount of C-reactive protein. All these changes are nonspecific and reflect the development of inflammation in the body.
Treatment of paraproctitis
Direct surgical intervention is the most important and main treatment method for both acute and chronic paraproctitis. If an abscess is present, it is immediately opened, its contents are completely removed and drainage is installed, which is necessary to ensure the constant removal of pus from the abscess. Moreover, for any such operations in the anorectal area, complete anesthesia of the operating area is required, since it is necessary to relax all the muscles. Most often today, sacral or epidural anesthesia is used, which allows you to completely get rid of sensitivity in the desired area, but in some cases general anesthesia may be required. For example, if complications develop or if infection is suspected, the surgeon and anesthesiologist may decide whether general anesthesia is necessary.
Pathological fistulas and other communications (both in acute and chronic forms) are also excised in order to clean and remove the contents, after which normal anatomy is restored. It is known that the earlier the operation is performed, the better the outcome and the faster the patient’s recovery. Sometimes the operation is immediately impossible due to the extremely high degree of inflammation and infection. In such situations, conservative treatment is first prescribed, and only later surgical operations are resorted to. In addition to the above, it must be remembered that any operation can, in rare cases, lead to undesirable consequences. After operations in the anorectal region, for example, fecal incontinence may be observed for some time or permanently.
In addition to surgical treatment, medications from the group of antibiotics are mandatory, which significantly shorten the period of illness and prevent the development of complications. Antibiotics destroy the immediate cause of the development of paraproctitis - bacteria that enter the peri-rectal tissue from the lumen of the rectum. In this case, broad-spectrum antibiotics are used, since the disease is usually caused by a mixed intestinal microflora, including different types of microorganisms. In addition to antibiotics, non-steroidal anti-inflammatory drugs (for example, ibuprofen or diclofenac) are also prescribed to reduce the intensity of pain and reduce the severity of the inflammatory process. Local therapy is used: ointments and creams with an antibacterial effect.
Complications of paraproctitis and prognosis of the disease
If medical care is not provided in a timely or incorrect manner, serious complications of acute paraproctitis may develop, which include:
- the occurrence of chronic paraproctitis, which is much more difficult to treat. In the chronic form of the disease, fistula canals are formed that connect the rectum to the skin. Closing these canals requires more complex surgery.
- the formation of phlegmon when an abscess breaks through with infection and purulent melting of large areas of surrounding tissue. To treat phlegmon, long courses of antibiotics are necessary. In addition, phlegmonous inflammation is much more often generalized.
- breakthrough of the abscess into the surrounding hollow organs (for example, into the vagina, rectum or organs of the genitourinary system) with the formation of pathological messages and the development of inflammation in these organs.
- the development of inflammation of the peritoneum (peritonitis), in which there is a widespread infection with an extremely high probability of an unfavorable outcome.
- the development of sepsis (a generalized infectious-toxic disease in which microorganisms enter the blood and spread throughout the body). Sepsis and peritonitis are the most severe complications of paraproctitis, directly threatening the patient's life.
If timely and correct medical care is provided, the prognosis of the disease is favorable. In order to cure paraproctitis in a timely manner and prevent the development of the listed complications, if symptoms appear, you need to consult a doctor as soon as possible.
Are there traditional methods for treating paraproctitis?
As mentioned earlier, the basis of treatment for both acute and chronic paraproctitis is the surgical method. Most often, paraproctitis cannot be cured without surgery. In addition to this, paraproctitis is caused by bacteria, against which antibiotic drugs are prescribed. Using enemas or suppositories made with herbs or other folk remedies may not only be ineffective, but also lead to further injury and complications. Also, you should not self-medicate by taking antibiotics without a doctor’s prescription. This can lead to further spread of infection and the development of resistance in the microorganisms that caused the disease.
Prevention of paraproctitis
There are no specific ways to prevent paraproctitis. However, you can avoid the action of predisposing factors, thereby reducing the likelihood of developing the disease:
- It is extremely important to prevent the occurrence of cracks and injuries to the rectum, the most common cause of which is constipation. It is important to maintain a proper diet, consuming enough foods containing fiber (plant foods). In addition, if you experience persistent constipation, you should consult a doctor to prescribe the necessary treatment.
- It is necessary to promptly treat acute infections of other organs and tissues to prevent the possible spread of microorganisms.
- In addition to constipation, persistent diarrhea can also cause rectal injuries. If you have loose stools for a long time, you should consult a doctor.
- If you have any chronic diseases of the perianal space, anal canal or rectum, they need to be treated promptly. The most common disease is hemorrhoids, which is also associated with stool disorders.
- To prevent the development of sexually transmitted diseases, which can also lead to acute paraproctitis, it is necessary to use personal protective equipment with each sexual contact.
How does acute paraproctitis become chronic?
In acute paraproctitis, as the tissue melts and the size of the abscess increases, the patient's condition gradually worsens. Then the abscess breaks through - a fistula is formed, and the pus comes out. The patient's condition improves and symptoms subside. Sometimes recovery occurs after this. In other cases, the fistula remains - feces and gases are constantly introduced into it, due to which the inflammatory process is maintained.
Reasons for the transition of acute paraproctitis to chronic:
- lack of adequate treatment;
- the patient contacting a doctor after the abscess has opened;
- medical errors, insufficiently effective treatment.
Diagnosis of paraproctitis
The clinical picture and examination by a coloproctologist play an important role in making a diagnosis. To clarify the location and size of the abscess, a digital rectal examination may be required, which, due to pronounced pain, is performed with the use of anesthesia. Additional tests may also be necessary.
Basic diagnostic methods:
- examination and digital examination;
- anoscopy;
- sigmoidoscopy;
- ultrasound examination using a rectal probe;
- fine needle puncture.
1 Operation for paraproctitis
2 Operation for paraproctitis
3 Operation for paraproctitis
Possible complications
Paraproctitis is a rather dangerous disease, as it occurs with the obligatory formation of a purulent abscess. Doctors identify several possible complications of the disease in question :
- purulent melting of the layers of the intestinal wall;
- release of feces into the perirectal tissue;
- breakthrough of pus into the retroperitoneal space;
- peritonitis.
Most often, the listed complications end in the development of sepsis - infection entering the bloodstream, which can actually lead to death for the patient.
And even if a purulent abscess has already formed, but its breakthrough occurred independently, then its contents end up in the area of the perineum and anus. It seems to the patient that all the pus has come out, especially since his state of health is dramatically improving. But in fact, in the absence of proper cleaning of the abscess and installation of drainage, there is a high probability of the formation of a repeated purulent abscess or fistula.
Complications of chronic paraproctitis include:
- deformation of the anal canal area;
- rectal deformity;
- changes in scarring on tissues;
- incomplete closure of the anal passage;
- pathological scarring of the walls of the anal canal;
- leakage of intestinal contents.
Important: if a fistula exists long enough, its tissue cells can degenerate into malignant ones. Doctors say that 5 years of regular relapses and progression of paraproctitis fistula is enough to diagnose cancer.
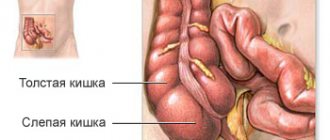
Anatomy of the rectum
In order to better understand the pathogenesis of the disease, it is necessary to know a little about the anatomical features of this area.
The rectum is the final section of the large intestine. Its length is about 15 cm. Anatomically, it is divided into the ampulla and the anal canal, which ends with the anus. Histologically, the rectum is represented by a mucous membrane, a submucosal layer and a muscular layer.
In the distal part of the intestine, the mucous membrane forms Morgagni columns; in appearance they look like vertical folds. Between these folds, depressions are formed, which blindly end in a small pocket called the crypt. Particles of feces or small foreign bodies can sometimes be retained in these crypts, which leads to purulent paraproctitis.
The rectum is surrounded by a lot of fiber. There are several cellular spaces in this area.
- The ischiorectal space is between the rectum and the ischium.
- The pelvic-rectal space is on the border with the abdominal cavity, above the pelvic floor muscles.
- Posterior rectal space - posterior to the rectum.
- Submucosal space - in the wall of the rectum, in the submucosal layer.
Diagnostics
Diagnosis of subcutaneous paraproctitis is quite simple - due to the pronounced symptoms of the disease. In this case, only a digital examination is carried out, and the finger is carefully inserted into the rectum and guided along the wall opposite to the one on which the abscess was localized. The diagnosis in this case is made based on the patient’s complaints, external and digital examination. Other methods for studying paraproctitis, incl. instrumental ones are not used due to increased pain in the anal area.
To determine ischiorectal paraproctitis, they often also dispense with only a digital examination, which usually reveals a thickening at or above the anorectal line and increased pain when examining a jerking character from the perineum. Instrumental diagnostic methods are used in extreme cases.
Paraproctitis formed under the rectal mucosa is also examined.
An abscess that occurs in the pelvic-rectal form of the disease can only be recognized by digital examination, but given the severity and depth of the inflammation, in some cases ultrasonography (ultrasound) or sigmoidoscopy (examination using a special device that is inserted into the anus) is used.
Signs of paraproctitis
The following symptoms are characteristic of this disease:
- sharp pain in the anus, aggravated by walking, coughing, physical effort, during bowel movements and just sitting;
- bowel and urinary disorders (constipation, pain when urinating);
- pain that can manifest itself in the perineum, anus, or lower abdomen;
- deterioration in general condition, weakness, chills, increased body temperature to 38-39 degrees, aching joints, lack of appetite;
- redness, thickening and swelling of the skin in the anus;
- pain, burning and itching in the anal area;
There are acute and chronic paraproctitis (occurs as a result of untreated acute paraproctitis, its improper or spontaneous opening) . In half of the cases, acute paraproctitis becomes chronic.
Treatment of paraproctitis
Paraproctitis requires surgical treatment. Immediately after the diagnosis of acute paraproctitis is established, it is necessary to perform an operation to open and drain the purulent focus. Since muscle relaxation and high-quality pain relief are important factors, complete anesthesia of the operating area is necessary. The operation is currently performed under epidural or sacral anesthesia; in some cases (if the abdominal cavity is affected), general anesthesia is given. Local anesthesia is not used when opening perirectal abscesses.
During the operation, a collection of pus is found and opened, the contents are pumped out, after which the crypt, which is the source of infection, is found and it is excised along with the purulent tract. After complete removal of the source of infection and high-quality drainage of the abscess cavity, you can count on recovery. The most difficult task is opening the abscess located in the pelvic cavity.
In case of chronic paraproctitis, the formed fistula must be excised. However, surgery to remove a fistula during the period of active purulent inflammation is impossible. First, the existing abscesses are opened, thorough drainage is performed, and only then can the fistula be removed. In the case of infiltrated areas in the canal, a course of anti-inflammatory and antibacterial therapy is prescribed as preoperative preparation, often combined with physiotherapeutic methods. It is advisable to carry out surgical intervention to remove the fistula tract as quickly as possible, since recurrence of inflammation and suppuration can occur quite quickly.
In some cases (senile age, weakened body, severe decompensated diseases of organs and systems), surgery becomes impossible. However, in such cases, it is advisable to treat pathologies using conservative methods, improve the patient’s condition and then perform surgery. In some cases, when the fistula tracts close during long-term remission, the operation is postponed, since it becomes problematic to clearly identify the canal to be excised. It is advisable to operate when there is a well-visualized landmark - an open fistulous tract.
Chronic paraproctitis
The cause of chronic paraproctitis is a relapse of acute paraproctitis. The disease has a purulent-fistula form.
In chronic paraproctitis, the abscess does not heal completely, and a fistula appears in its place. At the slightest stress (as a result of constipation or physical exertion, for example), inflammation develops again, sometimes in a different place of the perineum, and re-infection occurs.
During the development of chronic paraproctitis, the fistula opening may close, pus may be retained, abscesses may occur, pus will break through and leak into the rectum, and necrotic tissue changes will occur. A whole branched system of fistulas with a large number of holes may appear.
Postoperative period at home
The basis for a successful recovery is proper nutrition in the postoperative period. It should include:
- In the first 3 days after surgery, the diet should be low-calorie, slag-free. Patients are allowed to eat porridge with water (rice, manna), steamed cutlets, omelettes.
- Then the diet can be expanded by adding boiled vegetables, baked apples, and fermented milk products.
- Spicy, salty, fatty foods and alcohol are completely prohibited. You should avoid raw vegetables, legumes, cabbage, baked goods and carbonated drinks.
- Coffee, tea, chocolate are completely excluded.
If the postoperative period passes without complications, of course, the patient can go home, and he can carry out dressings independently. To do this you need:
- treat the wound with hydrogen peroxide;
- wash it with an antiseptic (furacilin, dioxidin);
- apply a sterile napkin with antibacterial ointment (you can use, for example, Levomekol).
In addition, after each act of defecation, it is necessary to carry out toileting of the postoperative wound and hygiene procedures. It is advisable to carry out sitz baths with herbal decoctions (calendula, dandelion, sea buckthorn), as well as replace the transportation material. After each stool, a thorough toilet of the perineum is necessary, sitz baths and a new dressing are desirable. You should definitely notify your doctor if you have stool retention in order to carry out cleansing microenemas.
It is recommended to use sanitary pads in the first days, since purulent discharge and local remedies can stain underwear.
If it is not possible to provide adequate wound care and care, you should go to a clinic (surgical office), where qualified specialists will be able to provide the necessary assistance.
At home, you will have to continue taking the following types of medications:
- antibacterial drugs;
- anti-inflammatory drugs;
- painkillers.
Usually paraproctitis heals after surgery within 3-4 weeks.
Causes
The causative agent of paraproctitis is intestinal flora; it is usually of a mixed nature and is represented by aerobic microorganisms. In descending order, the frequency of detection of pathogens can be presented in the following order:
- staphylococci (up to 70%);
- streptococci (up to 60%);
- E. coli (about 50%);
- proteus (24%);
- clostridia (7-10%)
Paraproctitis caused by only one pathogen (specific) occurs only in 1-2% of all cases.
Predisposing factors for the development of paraproctitis are:
- Immunosuppressive conditions. They occur against the background of HIV infection, indiscriminate use of broad-spectrum antibacterial drugs, glucocorticosteroids, and cytostatics.
- Disorders of immune reactions during acute inflammatory diseases (acute respiratory infections, influenza, sepsis, colitis, enteritis, etc.).
- Reduced tissue trophism in obliterating atherosclerosis or diabetes mellitus.
- Hemorrhoids in the acute stage.
- Cracks and other mechanical damage to the rectum and anal area.
Violation of the integrity of the mucous membrane, combined with a decrease in local protective factors, promotes the migration of microbial agents through the glandular ducts into the perirectal tissue. Usually, the space between the external and internal sphincter, the blinking crypt, is additionally affected. In severe cases, fistulous tracts may appear, opening in the skin of the paraanal area or into other organs (bladder, uterus, etc.).
Diet
There is no special diet for paraproctitis. But, for a quick recovery, you must follow a diet that consists of the following recommendations:
- Try to eat according to a schedule, at least 4-5 times a day, at approximately the same time.
- It is necessary to take hot food at least once a day (at lunch): soup, broth.
- It is better to make dinner light, limit meat products and large amounts of carbohydrates in the evening.
- It is better that all foods are low-fat: lean meats, chicken breast, turkey, lean fish.
- It is better to steam, boil or bake, but limit the consumption of food fried in vegetable or butter and other fats.
- Soups and broths should be weak, secondary, and it is better to cook soups in vegetable broths. If you want to make meat or fish soup, then these products are boiled separately and added to the finished dish.
- Drink enough water: at least 1.5 liters per day.
What can you eat if you have paraproctitis?
- sauerkraut;
- carrots in any form;
- tomatoes, cucumbers, radishes;
- onions, green onions, spinach;
- boiled beets;
- fruits of trees and shrubs;
- dairy products;
- low-fat steamed meat and fish dishes;
- black bread;
- light soups;
- cereals (except rice);
- fruit, berry and herbal decoctions;
- infusions of prunes, lingonberries and rose hips.
Prohibited products:
- rice and semolina;
- strong brewed tea, coffee, cocoa;
- chocolate;
- flour products, including pasta;
- cereals;
- spicy, smoked, sour, fatty;
- white flour bread;
- fatty foods;
- fast food;
- alcohol.
Diagnosis of acute subcutaneous paraproctitis
Diagnosis of acute subcutaneous paraproctitis begins with a conversation with a doctor. Often patients turn to a general surgeon or proctologist. The specialist clarifies the patient’s complaints in detail, clarifies their nature and time of occurrence. Additionally, he asks about concomitant diseases and their treatment, and the constant use of any medications.
During the questioning, special attention is paid to pathologies of the gastrointestinal tract: Crohn's disease, ulcerative colitis, the presence of hemorrhoids and anal fissures, the occurrence of gastric bleeding or the appearance of blood during or after defecation. It is important for your doctor to be aware of the potential for allergic reactions to medications.
Next, the site of the disease is examined. According to its results, characteristic symptoms of paraproctitis are revealed in the form of a large hyperemic swelling, often with a white purulent dot. This area is surrounded by a dense hot infiltrate of edematous tissue. During the examination, the doctor additionally notes the presence or absence of cracks and hemorrhoids.
Palpation for paraproctitis consists of a digital examination of the rectal cavity. The doctor determines the presence of a dense, extremely painful and edematous abscess.
Sometimes, with a widespread purulent inflammatory process, a special research method is used, such as fistulography. This is an x-ray examination, with the help of which the location, size of the inflammatory focus, and the course of spread of pus are clarified, using radiopaque substances.
In especially severe cases, ultrasound diagnostics is performed. It also provides information about the shape, boundaries, the presence of pockets and streaks and their exact location.
At the same time, a clinical blood test is performed. With subcutaneous paraproctitis, the erythrocyte sedimentation rate and the number of leukocytes are increased, and to a greater extent their neutrophil fraction.
Specialists at the Yusupov Hospital use modern methods for diagnosing paraproctitis. A special feature of the approach is the complete absence of discomfort due to the use of painkillers.
We use professional, reliable equipment and individually study the medical history of each patient.
Prevention
The main task after recovery is to prevent relapse of paraproctitis. Prevention consists of the following measures:
- eliminating constipation;
- a diet that ensures the establishment of regular, light stools;
- maintaining optimal weight;
- getting rid of hemorrhoids and anal fissures;
- careful hygiene, washing with cool water after each bowel movement;
- destruction of chronic foci of infection in the body;
- treatment of major diseases (diabetes mellitus, atherosclerosis, gastrointestinal diseases, etc.)
Risk factors
There are several factors that increase the risk of developing a perirectal abscess, these include:
- Diabetes mellitus of any degree of compensation (see blood glucose norm)
- Immunodeficiency (see symptoms of HIV, what is immunity)
- Vascular atherosclerosis (see how to reduce cholesterol without drugs)
- Anal intercourse
- Presence of hemorrhoids (see internal hemorrhoids)
- Constipation (see laxatives for constipation)
- Presence of chronic anal fissures (see treatment of anal fissures)
Prognosis for paraproctitis
A favorable prognosis in the treatment of acute paraproctitis is quite possible. However, this will require timely diagnosis and treatment. Therefore, it is extremely important that the patient consult a doctor immediately after identifying the first symptoms of the disease. Otherwise, if the disease is not treated for a long time, serious complications for the patient’s health may occur. In particular, ignoring the symptoms of pathology can lead to the formation of fistulas and the progression of the disease to an acute form.
After surgery, during which the fistulas were excised, the patient recovered completely. However, it is worth noting that excision of fistulas located quite high can be problematic. In some cases, fistula tracts cause the spread of purulent inflammation into hard-to-reach areas of the pelvis, which ultimately causes partial removal of the infection and, as a consequence, relapse of the disease. If during the operation the abscess was only opened without removing its connection with the intestinal lumen, complete recovery is unlikely.
This is due to the fact that the patient develops a rectal fistula, after which after some time the disease relapses.
Rectal fistula Rectal cancer Proctitis Hemorrhoids Ulcerative colitis of the intestine A lump has appeared in the anus - what could it be?
Treatment
Photo: garmonia-med.su
The main method of treating paraproctitis is surgical intervention, which is performed when the main symptoms of the disease have weakened, that is, after the acute period has stopped. During surgery, the abscess is opened and then drained, which is necessary to ensure the outflow of the abscess contents. The fistula canal, if any, is also surgically removed. Neglecting the timing of the operation is strictly prohibited, since early surgical intervention is the key to the patient’s complete recovery. It is important to understand that the absence of surgical treatment will inevitably lead to an exacerbation of the disease. That is why it is strongly recommended to immediately consult a specialist when the first symptoms of paraproctitis appear.
Antibiotics and non-steroidal anti-inflammatory drugs (NSAIDs) are prescribed as medications. The action of antibacterial drugs is aimed at destroying pathogenic microflora, which is necessary in the treatment of paraproctitis. In addition, their use helps prevent the spread of the infectious process. Non-steroidal anti-inflammatory drugs not only reduce the severity of the inflammatory process, but also have an analgesic effect, which plays an important role in relieving the pain syndrome that worries the patient with paraproctitis.
Physiotherapeutic treatment can also be used during remission of the disease. For paraproctitis, the following are used:
- UHF therapy is a method of physiotherapeutic treatment based on the effect of a high-frequency electromagnetic field on the human body. It has an anti-inflammatory effect and also improves lymph and blood circulation at the site of exposure;
- microwave therapy is a type of physiotherapeutic treatment that involves the use of ultra-high-frequency electromagnetic oscillations for therapeutic purposes. Has a local anti-inflammatory effect;
- infrared irradiation - the method is based on the use of infrared radiation or infrared rays. It has an anti-inflammatory effect, improves tissue regeneration, and provides local tissue resistance to the effects of an infectious agent.
As you know, any disease is easier to prevent, which is why it is recommended to follow the following preventive measures:
- Use a rational and balanced diet. Particular attention should be paid to eating enough fiber-rich foods every day. You should also refrain from eating fatty, fried and smoked foods. In addition, it is necessary to give up bad habits, in particular smoking and drinking alcohol;
- Observe the rules of personal hygiene of the perineum and anus, including not forgetting to regularly wash after each bowel movement;
- Treat constipation and anal fissures of the rectum in a timely manner.
What is dangerous about acute paraproctitis: complications
Acute paraproctitis is included in emergency surgery. The doctor has no right to postpone the operation until the morning or for several hours. This is considered a blunder in tactics. A violent purulent process in the peri-rectal tissue causes necrosis of adjacent tissues. The zone is spreading every hour. Melting of the intestinal wall causes fecal peritonitis, sepsis with high mortality.
In order to provide timely assistance and diagnose, proctologists train general surgeons, so the operation can be performed in any surgical hospital. Refusals, hopes for traditional methods of treatment, and delays in qualified intervention lead to unforgivable complications and dramatically worsen the condition of patients.
Bibliography
- Vorobyov G.I., Koplatadze A.M., Bolkvadze E.E. The choice of method of surgical treatment of patients with complex forms of acute recurrent paraproctitis. Current issues in coloproctology. 1st Congress of Coloproctologists of Russia. Samara, 2003. Pp. 45-46.
- Charyshkin A.L., Dementyev I.N. Results of treatment of patients with acute paraproctitis. Basic research. 2013 No. 2, 7. Page. 428-431.
- Lavreshin P.M. An integrated approach to the treatment of acute paraproctitis. Current problems of coloproctology. V All-Russian conference with international participation. Rostov-on-Don, 2001. Pp. 44.
- Kamaeva D.K., Koplatadze A.M., Kim S.D., Bolkvadze E.E., Egorkin M.A., Kuznetsov N.Yu. Treatment of patients with acute paraproctitis using the latex ligature method. Surgery. Journal named after N.I. Pirogova, 2000 No. 10. Page. 31-34.
Paraproctitis in children
The course of paraproctitis in children can be characterized by the same symptoms as in adults: high fever, muscle and joint pain, intoxication, loss of appetite.
Paraproctitis in children often manifests itself in a subcutaneous form. The most common causative agent of the disease in infants is staphylococcus, which penetrates through diaper rash and causes the occurrence of a subcutaneous type of illness.
Important! Weakened immunity, combined with an imbalanced intestinal microflora, increases the likelihood of paraproctitis in children many times over.
Video about complications of paraproctitis in children
Forms and symptoms
Acute type of disease
Symptoms of acute paraproctitis are pronounced and fully manifested. In acute cases, rectal fistulas form, causing discomfort. The deviation begins with the following manifestations:
A symptom of the disease may be lack of normal sleep.
- painful sensations in the butt, aggravated by excretion of feces;
- a febrile state in which the body temperature rises;
- impaired bowel movement, in which constipation alternates with diarrhea;
- frequent urge to go to the toilet, which is most often false;
- signs of intoxication:
- general malaise;
- constant desire to drink;
- lack of normal sleep;
- painful sensations in the head.
As the abscess develops, it often ruptures, which can result in bleeding from the anus. Pus is often excreted along with feces, and when the abscess breaks through to the skin, a noticeable fistulous tract is observed. In this case, the symptoms subside a little, but the treatment of paraproctitis becomes more complicated.
Chronic
If treatment for an acute disease is not started in time, then chronic paraproctitis cannot be avoided. In a chronic course, the pathology recurs several times even after drug treatment. In this case, the same signs are noted as in the acute course, but they may not be expressed so clearly or may not manifest themselves fully. The patient experiences a constant increase in temperature, which is difficult to control with antipyretics. Without surgery, it will not be possible to eliminate this form of deviation.
Stages of development
In a chronic course, there are 2 stages of paraproctitis, each of which manifests itself with special symptoms:
In the acute course of the disease, fatigue is a characteristic condition for a person.
- Exacerbation. It is characterized by inflammation of superficial fistulas, inside which purulent fluid accumulates. During this period, a person looks very tired and painful, since paraproctitis affects the general condition.
- Remission. This phase is characterized by an improvement in the general condition of the patient. However, complete recovery does not occur; the pathology may recur.
During the acute stage, the patient complains of the following manifestations:
- pain in the rectal area;
- inflammation, which causes the temperature to rise;
- bleeding from the anus after rupture of the fistula;
- gas incontinence due to damage to the sphincter muscle.
In males, potency often decreases during the acute stage.