Rheumatism is an inflammatory infectious-allergic systemic pathology that affects connective tissue structures. The leading clinical manifestations of the disease are elevated body temperature and multiple symmetrical arthralgias of a volatile nature. Rheumatism is characterized by both simultaneous and sequential involvement of several joints in the pathological process. The main reason for the development of the disease is an inadequate response of the immune system to the introduction of certain pathogenic microorganisms.
In the diagnosis of rheumatism, the most informative are serological and bacteriological studies: determination of the level of C-reactive protein, detection of elevated antibody titers. To determine the extent of joint damage, radiography, MRI, and CT are performed. Treatment is conservative using immunosuppressants, glucocorticosteroids, and non-steroidal anti-inflammatory drugs.
Pathogenesis, causes, provoking factors
Rheumatism of the joints is most often diagnosed in children and adolescents aged 7-15 years. Representatives of the weaker sex are most susceptible to developing pathology. The pathology affects not only the musculoskeletal system, but the serous membranes, skin, cardiovascular and central nervous systems. When studying the etiological aspects, a relationship was discovered between the occurrence of rheumatism and the previous penetration into the body of pathogens of scarlet fever, tonsillitis, pharyngitis, erysipelas, and otitis media. These group A beta-hemolytic streptococci provoke the development of an inflammatory process. They release toxic products of their vital activity into the surrounding space, which leads to the appearance of symptoms of general intoxication.
More than 95% of people with streptococcal infections fully recover after a course of antibiotic therapy and acquire lasting immunity to pathogens. The remaining infected people do not develop a full-fledged immune response. Therefore, with the repeated penetration of beta-hemolytic streptococci, the development of a complex autoimmune inflammatory reaction is observed. The role of provoking factors are:
- a sharp decrease in immunity;
- being in large groups during an unfavorable epidemiological situation;
- unbalanced diet, lack of foods high in microelements, fat- and water-soluble vitamins;
- frequent hypothermia;
- aggravated medical history, including family history.
After the introduction of infectious agents into the body, the immune system produces a large number of antistreptococcal antibodies - antistreptolysin-O, antistreptohyaluronidase, antistreptokinase, antideoxyribonuclease B. Immune complexes begin to rapidly form from immunoglobulins, streptococcal antigens, and components of the complement system. They circulate in the bloodstream, spreading throughout the body and settling in connective tissue structures. Where immune complexes are localized, aseptic autoimmune inflammatory processes are launched. Streptococcal antigens are characterized by pronounced cardiotoxic properties, so most autoantibodies are formed to the heart muscle. The recurrent, progressive course of joint disease is caused by repeated infection, stress and depression, and hypothermia.
| Forms of rheumatism | Characteristic features of the development of pathology |
| Acute | A rheumatic attack occurs suddenly, all symptoms are pronounced. Characterized by polysyndromic (involvement of all organs) lesions, high activity of the inflammatory process. The therapy performed is highly effective |
| Subacute | The relapse can last up to six months. Clinical manifestations are of moderate severity, attack activity is moderate. The result of treatment depends on the state of the patient’s immunity |
| Protracted | A rheumatic attack lasts more than 6 months. Its dynamics are sluggish, inflammation activity is low. Signs of damage can appear only from the musculoskeletal system. When carrying out diagnostic measures, only a previously formed heart defect is usually detected, and new signs of joint damage are still absent |
| Recurrent | Clinical manifestations are polysyndromic; damage not only to joints, but also to internal organs progresses rapidly. Characterized by an undulating course with frequent painful relapses |
How to prevent the disease?
For this purpose, primary prevention measures have been developed, including:
- avoidance of people suffering from streptococcal pathology (tonsillitis, pharyngitis, scarlet fever, erysipelas);
- strengthening your own immune forces - an active lifestyle, hardening, staying in the fresh air, a full night's sleep (preferably from 22 to 6 am), a healthy diet, including adequate protein, fresh fruits and vegetables;
- combating high overcrowding in boarding schools, schools, colleges and public institutions;
- timely treatment of acute and chronic infections caused by beta-hemolytic streptococcus, including the prescription of the following antibacterial drugs: Amoxicillin, Augmentin, Clarithromycin, Roxithromycin or Clindamycin, Lincomycin in case of resistance to the first four drugs or their individual intolerance.
And secondary prevention , aimed at preventing repeated rheumatic attacks. It comes down to the prescription of prolonged forms of Benzathinebenzylpenicillin - Retarpen, Extensillin, Bicillin-5:
- in persons who have suffered a rheumatic attack without carditis - for five years;
- those who have had carditis without a heart defect - ten years;
- with various defects - for life.
The use of prolonged forms significantly improves the quality of life of patients with rheumatism and minimizes the development of further life-threatening complications.
But, unfortunately, at the moment there is no ideal scheme that completely destroys streptococcal infection.
Clinical symptoms and differences between rheumatoid and rheumatoid arthritis
With rheumatism, signs of joint damage occur in 20% of examined patients. Many pathologies of the cardiovascular system manifest themselves as pain in the heart, and arthralgia is quite specific and directly indicates the development of an inflammatory process in the joints. The clinical picture of rheumatism is similar to the symptoms of rheumatoid arthritis. They occur 7-14 days after an infection has already been suffered - pharyngitis, scarlet fever, tonsillitis. That is, a person considers himself completely healthy when his condition sharply worsens again. Body temperature rises to 39°C, he complains of weakness, fatigue, headaches, suffers from excessive sweating, chills.
Unlike rheumatoid arthritis (which greatly facilitates diagnosis), it initially affects not the small metatarsophalangeal joints of the hands and feet, but the large joints - ankles, knees, shoulders, elbows. The nature of arthralgia is multiple, symmetrical and volatile. This means that several paired joints are affected at once, and pain is felt throughout the day in different joints. The main symptoms of rheumatism include:
- swelling and swelling of the joints, especially in the morning;
- redness of the skin over the joint, hyperemia;
- a sharp decrease in range of motion, stiffness;
- the formation of dense, round, painless, inactive nodules localized to the joint area;
- The severity of pain increases with increased physical activity or lifting heavy objects.
The pathology in most cases is benign. Even an acute inflammatory process does not provoke damage to cartilage, bone, and connective tissue joint structures. There is no deformation of the joints, but moderate pain persists for quite a long time.
Symptoms are most intense at the beginning of a rheumatic attack due to increased body temperature and fever. A specific aches in the joints arise, aching, dull, pressing, “gnawing” pain appears that does not subside at night. The similarity between rheumatism and rheumatoid arthritis lies in the obligatory presence of extra-articular symptoms. The general state of health worsens, the functional activity of some vital systems decreases. With rheumatism, the membranes of the heart become inflamed, interruptions in the functioning of the heart occur, and in especially severe cases, patients are diagnosed with circulatory failure. One of the complications is chorea, which manifests itself in involuntary muscle twitching.
General information about the disease
Rheumatism, or rheumatic fever, is characterized by a chronic course and a tendency to relapse. The disease, which usually occurs as a complication of tonsillitis or pharyngitis caused by group A streptococcus, affects large joints and the heart. In severe cases, rheumatism leads to the development of heart defects that threaten the patient's life. The classification of rheumatism is broad, that is, the disease manifests itself in many forms and stages. In any case (even if the joint pain has disappeared or become less intense), the pathology requires complex and ongoing treatment under the supervision of a rheumatologist and cardiologist.
Diagnosis of rheumatism
The primary diagnosis is made based on the patient’s complaints, external examination, and medical history. A recent streptococcal infection is a definite clue. When conducting bacteriological studies, an increased titer of antibodies produced by the immune system to destroy pathogenic bacteria is established. These are antistreptolysin, antistreptokinase, antihyaluronidase. A biological sample taken from the throat is inoculated into nutrient media. The stage of the inflammatory process is determined by the number of formed colonies. The final diagnosis is made after detecting the following diagnostic criteria for rheumatic fever:
- polyarthritis - damage to several joints;
- presence of subcutaneous nodules;
- ring-shaped erythema is a polyetiological disease of the skin;
- clinical manifestations of carditis, chorea;
- joint pain due to fever;
- increased blood sedimentation rate, leukocytosis, the presence of C-reactive protein in a general blood test;
- prolonged P–Q interval on the electrocardiogram.
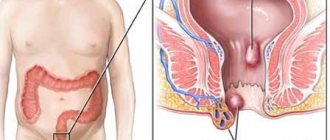
An example of damage to the hip joint.
X-rays, CT, and MRI are performed to assess the condition of articular structures and exclude other inflammatory and degenerative pathologies.
Differential diagnosis with tuberculosis, neuroses, and nonspecific endocarditis is also necessary.
Clinical and anatomical lesions
When classifying rheumatism, the first (1) are the clinical manifestations, the state of the blood circulation and the general clinical and anatomical characteristics of the involvement of the heart or other body systems. In medical practice, a disease is distinguished with the development of heart disease or without it (lesions involving the heart), rheumatic lesions of the lungs, kidneys, neurorheumatism (the involvement of other systems is assessed).
In the WHO classification of rheumatism, clinical manifestations are divided into main and additional. The main ones are arthritis (a common inflammatory disease of the joints), chorea (involuntary movements beyond the control of the patient), carditis (inflammatory damage to the heart), subcutaneous rheumatic nodules (systemic inflammation of connective tissues), ring-shaped erythema (damage to the dermis, manifested by various rashes) . Additional ones include arthralgia (joint pain, which can be either transient or permanent), serositis (inflammation of the serous membrane, for example, the pleura, peritoneum or pericardium) and abdominal pain syndrome.
What happens if there is no treatment
Each stage of pathology lasts no more than 2 months. During each relapse, repeated tissue lesions occur in the area of the formed fibrous foci. In addition to the joints, the tissue of the heart valves is involved in the inflammatory process; numerous sclerotic changes occur in their valves. They begin to grow together, which significantly increases the likelihood of subsequent acquired heart disease. The following symptoms are characteristic of rheumatic carditis:
- strong heartbeat;
- pulmonary edema, shortness of breath;
- heart pain of varying intensity;
- increased fatigue, weakness;
- heart rhythm disturbance.
Rheumatic carditis is diagnosed most often in patients 14-25 years old. Its clinical manifestations may be minor, but severe damage to the heart valve can also be detected. Rheumatism causes disruption of the central nervous system, especially in children. This is expressed in moodiness, irritability, absent-mindedness, and apathy. In the future, problems arise with memorization, speech, and concentration. In adults and children, damage to the abdominal organs is possible. Abdominal syndrome develops - abdominal pain, nausea, vomiting occur.
Variants of the course of the disease
There are five types of rheumatism, depending on the course of the disease:
- latent;
- spicy;
- subacute;
- protracted;
- recurrent.
Acute rheumatism is characterized by suddenness and sharp severity of the clinical picture, a high degree of activity of the process, and rapid and effective treatment. In the subacute course, the duration of the disease is from three to six months, the symptoms are less pronounced, the effectiveness of treatment is less, and the activity of the process is moderate.
The protracted version of rheumatism occurs with sluggish dynamics, prolonged rheumatic attack, and low activity of the process. The latent course is characterized by the absence of instrumental and clinical laboratory data; the disease is diagnosed by an already formed heart defect. The continuously relapsing variant of development is determined by severe exacerbations and incomplete remissions, progressive damage to internal organs.
Treatment tactics
In case of acute joint pain that occurs against the background of disruption of the cardiovascular system, the patient is hospitalized. In other cases, treatment is carried out at home. Antibiotic therapy is indicated only if there are infectious foci in the body. During culture, the sensitivity of streptococci to antibacterial agents is determined, which becomes the main criterion for their selection. As a rule, treatment regimens include drugs from the penicillin group in the form of solutions for intramuscular administration. The duration of the therapeutic course depends on the degree of tissue infection.
Infectious agents.
To eliminate pain, non-steroidal anti-inflammatory drugs are used - Ibuprofen, Diclofenac, Celecoxib, Ketoprofen, Ketorolac, Meloxicam, Nise. You can get rid of mild arthralgia with the help of external agents Fastum, Nimesulide, Artrosilene, Finalgel.
If the pain is intense and does not subside for a long time, then NSAIDs are administered intramuscularly. The following drugs are also used to treat rheumatism:
- glucocorticosteroids Prednisolone, Hydrocortisone, Diprospan, Dexamethasone to eliminate acute inflammation and severe pain;
- immunosuppressants Azathioprine, Cyclosporine, Hydroxychloroquine to correct the immune response.
After stopping the inflammatory process, patients are prescribed warming ointments - Capsicam, Finalgon, Apizartron, Viprosal. They have an analgesic, anti-edematous, and blood circulation-improving effect. To prevent relapses of the pathology in the fall and spring, it is recommended to take NSAIDs in reduced dosages and in combination with proton pump inhibitors for a month.
The prognosis for complete recovery is favorable only with timely treatment, as long as the pathology does not affect the organs of the cardiovascular system. Therefore, it is necessary to seek medical help at the first clinical manifestations of rheumatism.
Complications
The classification of rheumatism takes into account the presence of complications. This is determined by the severity and recurrent nature of the disease. Adhesions may appear, mitral valve insufficiency, mitral stenosis, aortic insufficiency, myocardiosclerosis and other heart defects may develop (if the valves are involved, treatment and prognosis are determined by the type of rheumatic valvular rheumatism), thromboembolic complications are possible, that is, cerebral ischemia, infarction of the kidneys, retina, spleen . Deadly complications are decompensated heart defects and thromboembolism of the great vessels.
Prevention of ARF
Prevention plays a major role in preventing the disease. According to WHO recommendations, the prevention of rheumatism can be primary and secondary.
Primary prevention
This type of prevention involves preventing the primary disease of rheumatism. Includes a range of individual and social events. The main directions of such prevention are:
- Measures that are aimed at increasing a person’s natural immunity: hardening, a healthy lifestyle, good nutrition, etc.
- Carrying out a set of sanitary and hygienic measures that reduce the likelihood of GABHS infection in groups, especially in children's groups.
- Timely and effective treatment of acute, sluggish and chronic GABHS-associated pharyngeal infections (tonsillitis, pharyngitis).
When all conditions for primary prevention of rheumatism were met, a significant decrease in incidence was noted.
Secondary prevention
It is carried out for all patients. Its main goal is to prevent relapses (recurrence of the disease) in people who have already suffered ARF. It usually begins in the hospital after completing a course of antibiotic therapy with short-acting drugs.
To carry out such prevention of rheumatism, long-acting penicillin preparations are used.
The most commonly used benzathine is benzylpenicillin. It is used by intramuscular injections (shots) once every two to three weeks. The dosage of the drug and the duration of secondary prevention are determined by the doctor.
Rheumatism
Kasallikning turlari: rheumatismni tasniflash
Kechish tabiati biyicha rheumatism ўtkir va surunkali shaklda buladi:
- Otkir rheumatism . Rheumatismning bu shakli 20 yoshgacha bulgan odamlarda uchraydi. Rheumatism ўtkir shaklining қўzғatuvchi agents and streptococcus. Rheumatism boshdan kechirilgan yukori nafas yўllari infectionsi bilan birlashsa, alomatlarning kechikishi (odatda 14-21 kunlarda) qaid qilinadi. Otkir rheumatismning uziga hos hususiyati uning rivozhlanish tezligidir. Dastlab, bemorlarni shamollash va grippdagi kabi umumiy intoxication alomatlari bezovta kiladi. Ainan shu alomatlarning ўkhshashligi bu kasallikni darhol aniklashga imkon bermaidy. Bir muncha vaqt ўtgach carditis, polyarthritis, teri ustida toshmalar, basan teri tugunlari kabi uziga hos alomatlar sezila boshlaydi. Kasallikning ўtkir davri uch oygacha davom etadi. Airim hollarda ўtkir rheumatism 6 oigach davám etadi.
- Surunkali rheumatism . Rheumatismning surunkali shakliga kelsak, y tez-tez kaytalanishi bilan characterlanadi, khatto bemor uz vaktida tegishli davolashni olib borsa ham. Ainiksa, surunkali rheumatismning kuchayishi kuz-kish mavsumida tez-tez sodir buladi, chunki sovuk zhiddiy kuzgatuvchi omil hisoblanadi. Bundan tashkari, namlik yukori bulgan zhoylarda uzoq muddat turish (yoki yashash) kasallikning kuchayishiga yordam beradi. Koidaga kira, surunkali rheumatismning khuruzhi yiliga bir necha marta sodir buladi.
Surunkali rheumatism yetarlicha ogir shaklda kechib, bemorning khayot sifatini sezilarli darazada kamaitiradi. Bemorni bўgimlardagi azobli oғrik, shuningdek yurak soҳasidagi oғriklar bezovta kiladi.
Kay azo shikastlanganliga karab, rheumatism kuyidagi turlarga bulinadi:
- Rheumatismning yurak shakli . Kasallikning bu shaklida yurak mushaklari tasirlanadi. Bundai ҳolatda bemorlardagi oғriқlar bir-biridan farq qiladi: kimdadir yakkol oғrik, bośkalarda esa mўadil oғrik қayk қilinadi. Dastlabki boskichlarda rheumatismning yurak shakli deyarli namoyon bўlmaydi va faqat muayyan instrumental tadqiqotlar, masalan, EKG yordamida aniklanadi. Kasallikning sўnggi bosqichlarida oғir yurak shikastlanishi va ўtkir yurak yetishmovchiligirivozhlanadi, bu yurak mushakining kiskaruvchi kobiliyatining pasayishiga olib keladi.
- Rheumatismning bugim shakli . Rheumatismning bўgimli (articular) shaklida faqat bўgimlar yoki yurak bilan bўgimlar shikastlanishi mumkin. Odatda, rheumatism bўgim shakli katta bўgimlarga ta'sir kiladi va ohirgi boskichlarda pathologist zharyon kichik bugimlarni gam qamrab oladi. Sekin-asta bғgim khaltachasi va togailarning shikastlanishi rўy beradi. Kuchli ogrik tufayli, bemor shikastlangan bugimni harakatlantirishi kiyinlashadi. Bugim rheumatismining ўtkir shaklida yoki khuruz davrida tana harorati 39 °C ga kadar kutarilishi mumkin.
- Rheumatismning neurologist Shakli . Asab tizimining rheumatic shikastlanishi bugim va yurak shikastlanishidan kura kamrok uchraydi. Rheumatismning neurologist shaklida harakatlanish uchun zhavob beradigan bosh miya pustlogi huzhayralari shikastlanadi. Shu bois, bemor oёқ-қўllari yoki yuz mushaklarining ikhtiyorsiz harakatlari kaid qilinadi.
- Rheumatism ўpka shakli . Juda kamdan-kam hollarda kuzatiladi, rematismga oid barcha holatlarning tahminan 1-3% ini tashkil etadi. Odatda, rheumatism ўpka shakli ўzini bronchitis pleurisy shaklida namoen qiladi.
- Rheumatismning teri shakli . Kasallikning bu shakli teri toshmalari yoki uziga hos rheumatik tugunlar shaklida namoen bўladi. Kasallikning teri shakli rheumatismga chalingan bemorlar umumiy sonining 5 foizidan oshmaydi.
- Rheumatismning ophthalmologist Shakli . Kasallikning bu shakli faqat rheumatismning classic alomatari bilan birgalikda aniklanadi. Odatda, ophthalmologist Shakli kuzning tur pardasiga tasir qiladi. Rheumatismning ophthalmologist shakli kisman yoki tўlik kўrlikka olib kelishi mumkin.