Local therapist
Burnatskaya
Svetlana Nikolaevna
33 years of experience
Local therapist, occupational pathologist. Member of the Russian Scientific Medical Society of Therapists
Make an appointment
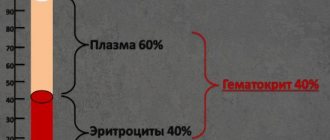
Agranulocytosis is a severe pathological condition. With it, there is a critical decrease in granulocytes in the blood. Granulocytes are an important fraction of the leukocyte series (neutrophils, eosinophils and basophils). At the same time, the concentration of basophils and eosinophils in the blood in the normal state is a small percentage, so changing their number does not have a significant effect. Thus, it can be argued that it is the decrease in the concentration of neutrophils that leads to the development of blood agranulocytosis. Hence the second name of the pathology – neutropenia.
Experts raise the question of agranulocytosis in a patient when the leukocytes in the blood decrease below 1×109/l and granulocytes below 0.75×109/l. Since leukocytes and granucolites perform a protective function against pathogens, a decrease in their concentration reduces the body’s ability to resist infections and viruses. The development of agranulocytosis is almost always accompanied by the development of various infectious processes, these can be ulcerative stomatitis or tonsillitis, pneumonia, hemorrhagic manifestations, etc.
Depending on the concentration of granulocytes, the severity of peripheral blood pathology is determined. The lower their concentration, the more severe the degree; there are three degrees: mild, moderate and severe. In severe cases, the granulocyte concentration is below 0.4 × 109/l.
In women, agranulocytosis is more common. In men, this disease is diagnosed on average 2-3 times less often. In most cases, the manifestation of pathology occurs after the age of 40 years.
Symptoms and signs
Since the pathology has several forms, the symptoms of agranulocytosis of different types differ. The immune type is characterized by acute agranulocytosis with the following symptoms:
- severe weakness and sweating;
- body temperature up to 39-40°C;
- pallor;
- the appearance of infectious stomatitis;
- inflammation of the pharynx and tonsils;
- inflammation of the gums;
- sore throat and spasm of the chewing muscles.
Myelotoxic and autoimmune types progress gradually and also gradually develop symptoms:
- hemorrhagic symptoms in the form of nosebleeds, bleeding gums, etc.;
- presence of blood in the urine;
- the occurrence of bruises, hematomas;
- abdominal pain and bloating, diarrhea if the intestines are affected;
- possible occurrence of chest pain when breathing.
Complications
Myelotoxic disease can have the following complications:
- sepsis (blood poisoning). Sepsis of the staphylococcal type is often observed. The most dangerous complication for the patient's life;
- perforation in the intestines. The ileum is most sensitive to the formation of through holes;
- pneumonia;
- severe swelling of the intestinal mucosa. In this case, the patient experiences intestinal obstruction;
- acute hepatitis. Often during treatment, epithelial hepatitis forms;
- formation of necrosis. Refers to infectious complications;
- septicemia. The more a patient suffers from a myelotoxic type of disease, the more difficult it is to eliminate its symptoms.
If the disease is caused by haptens or occurs due to a weak immune system, then the symptoms of the disease are most pronounced. Among the sources that cause infection are saprophytic flora, which include Pseudomonas aeruginosa or Escherichia coli. In this case, the patient experiences severe intoxication, an increase in temperature to 40–41 degrees. Pseudomonas aeruginosa can cause metastatic infectious ulcers on the body, which, when opened, can be found on the surface of the kidneys, lungs or other organs.
Causes
The occurrence of agranulocytosis can have different causes, depending on which the pathology is classified.
Types of illness
Myelotoxic agranulocytosis is the result of the influence of various unfavorable factors on the red bone marrow. Under their influence, deep depression occurs in the hematopoietic process responsible for the production of granulocytes. Unfavorable factors should be understood as internal diseases of the body and external adverse effects. Examples of external influences: poisoning with substances and poisons that suppress hematopoiesis (mercury, arsenic, benzene, etc.), radiation exposure, taking myelotoxic drugs. Among the diseases that most often cause agranulocytosis, experts identify acute leukemia, sarcoma and metastasis to the red bone marrow, and chronic myeloid leukemia.
Immune agranulocytosis is characterized by the destruction of granulocytes in the blood due to the occurrence of pathological immune reactions in the body. This type is further divided into the following forms of agranulocytosis.
- Autoimmune - occurs in most cases against the background of connective tissue diseases. These include, for example, rheumatoid arthritis or systemic lupus erythematosus.
- Hapten agranulocytosis or drug-induced agranulocytosis develops with the participation of haptens in immune reactions. Haptens themselves are harmless substances, but under certain situations and reactions they can cause the destruction of granulocytes. The role of haptens most often are drugs that the patient takes as part of the treatment of various diseases. Hence the second name of the pathology – “medicinal”.
- Genuine - this type is assigned to the patient in cases where diagnostics have not revealed the reasons for the decrease in granulocytes in the bloodstream.
Pathological anatomy
Pathological signs of agranulocytosis are necrotic-ulcerative changes, most often found in the oral cavity and pharynx. The tonsils are enlarged, loose, gray-dirty in appearance, with fibrinous deposits and ulcerations. In the area of the soft and hard palate, foci of necrosis are found, sometimes with perforation of the soft palate. Necrotic changes are detected in the skin, at injection sites, in the perineal area, and around the anus. Foci of necrosis are described in the conjunctival sac, in the mucous membrane of the larynx, esophagus and stomach. With the development of necrosis in the mucous membrane of the small or large intestine, including the appendix, intestinal bleeding and perforation are observed. Necrotic ulcers can be in the wall of the bladder, in the genitals, especially in the vaginal wall, as well as in the tissue of the liver and other organs. Microscopic examination shows that there are no neutrophilic leukocytes in areas of necrosis. The demarcation strip around the necrosis is not detected; lymphohistiocytic and plasma cell accumulations can be seen near the areas of necrosis. Pneumonia is fibrinous-hemorrhagic in nature. In this case, fibrinous deposits are also located on the pleura. In the area of pneumonia, areas of tissue decay (gangrene) may be detected. Microscopically, desquamated epithelial cells, bacteria, yeast cells and their mycelium are visible in the lumens of the alveoli. Lymph nodes are usually not enlarged. With necrotic changes in the oral cavity, a slight enlargement of the cervical and submandibular lymph nodes may be observed. Their microscopic structure is relatively preserved. In the cortex and especially in the area of the medullary cords, a large number of plasma cells are detected. Proliferation and swelling of reticuloendothelial cells in the sinuses is sharply expressed. The spleen is often unchanged. The spleen tissue is of a soft consistency; on the section there is a pink-gray pulp with a large scraping. Microscopic examination reveals a uniform decrease in the number of red pulp cells of the spleen. The bone marrow of flat bones is macroscopically more common than usual, somewhat dry, but there may be various foci of hemorrhage - from small to extensive; in the lower and middle third of the tubular bones, the bone marrow is fatty.
Microscopically, small foci of resorption of bone beams with the formation of small lacunae are revealed. Osteoblast proliferation may be observed in areas of bone resorption. The ratio of adipose and hematopoietic tissue is different. More often there is a decrease in the number of hematopoietic cells and an increase in the number of fat cells in the bone marrow. In the cellular composition, attention is drawn to a sharp decrease in the number of young, band and segmented granulocytes. There may be some predominance of young forms of granulocytes. Megacarpocytes and red row cells are usually preserved. In the most severe course of AGRANULOCYTOSIS, the picture of the bone marrow is the same as in hypoplastic anemia (see).
Risk factors
The risk group primarily includes patients who are frequently exposed to severe infections, as well as unusual, rare infections. Another risk group is patients who, as part of the treatment of other diseases, receive drugs or therapy (for example, radiation therapy), which can cause the development of agranulocytosis. Patients at risk should be especially attentive to their well-being and pay attention to alarm bells. Accurate laboratory diagnostics are required to confirm the diagnosis.
Classification
The gradation of types of agranulocytosis depends on a number of external factors, among which doctors identify the reasons for its appearance in the body and the path of subsequent development. Taking this into account, we can talk about the following types of disease:
- Myelotoxic.
- Immune (autoimmune and hapten).
- Genuinnom.
The essence of the first two of them will be discussed in the following sections. As for the third, genuine type of disease, this professional term means that doctors have not been able, despite all efforts, to establish the cause of the catastrophic decrease in the number of granulocytes in the blood.
Diagnosis of agranulocytosis in patients
If the patient is at risk or corresponding symptoms appear without other visible causes, agranulocytosis is diagnosed using the following methods.
- A general blood test is the very first and most important test that allows you to determine the concentration of granulocytes and leukocytes in the bloodstream.
- Antibody test - prescribed to identify autoimmune agranulocytosis, allows you to determine antineutrophil antibodies.
- Myelogram - allows you to determine the decrease in myelokaryocytes and other indicators of the condition of peripheral blood.
If necessary, when diagnosing agranulocytosis, other research methods are prescribed to determine the degree of damage to organs and systems caused by this pathology. In particular, the following may be prescribed:
- X-rays of the lungs;
- visiting a dentist;
- blood chemistry;
- blood sterility tests;
- consultation with an otolaryngologist.
Diagnosis
The diagnosis is made on the basis of anamnestic data, a characteristic clinical picture, data from a study of peripheral blood and bone marrow puncture. The diagnosis of immune AGRANULOCYTOSIS can be confirmed by serological studies: detection of anti-leukocyte antibodies (see Blood groups, leukocyte groups). AGRANULOCYTOSIS must be differentiated from acute leukemia in the aleukemic stage and hypoplastic anemia. In the first case, the decisive factor in diagnosis is the study of bone marrow puncture, the second is an indication of the suddenness of the development of AGRANULOCYTOSIS due to its immune nature or information about long-term use of drugs with myelotoxic action (sometimes interrupted several weeks before the development of AGRANULOCYTOSIS). Observation of the patient allows us to come to a final conclusion about the nature of bone marrow devastation.
Treatment
Once a diagnosis is made and the type of pathology is verified, treatment should begin immediately. In most cases, the patient requires hospitalization in the hematology department. This is necessary to create aseptic conditions. In the isolation ward, quartz treatment is carried out according to a schedule, and visits to the patient are also limited. Such measures are necessary to prevent the occurrence of additional infectious complications.
The specialist prescribes a comprehensive treatment for agranulocytosis to the patient, and it begins with eliminating the factors under the influence of which the development of this pathological condition began. The set of measures for the treatment of agranulocytosis includes:
- elimination of negative impact factors, including refusal to take myelotoxic drugs, various chemicals, etc.
- treatment and prevention of infectious diseases;
- enhanced oral care;
- steroid therapy;
- administration of immunoglobulin (intravenously);
- leukocyte transfusion;
- plasmapheresis, etc.
The range of therapeutic measures depends on the type of disease, its degree, as well as the degree of other pathologies present in the body. In each case, the treatment complex is prescribed individually.
Diet
Diet 13 table
- Efficacy: therapeutic effect after 4 days
- Time frame: no more than 2 weeks
- Cost of products: 1500-1600 rubles per week
If the number of neutrophils in the body is reduced, it is necessary to especially carefully monitor nutrition so as not to provoke complications dangerous to health. First of all, it is important to avoid those foods that could potentially contain germs or bacteria.
It is recommended to include the following foods in your diet:
- Pasteurized milk, yogurt, cheese.
- All types of meat and fish that have previously undergone thorough heat treatment.
- Hard-boiled eggs.
- Citrus fruits, bananas, frozen fruits.
- Porridge, pasta.
- Nuts.
Prevention
Doctors recommend a set of preventive measures, the basis of which is the prevention of infectious complications. Medicines whose use is prohibited include those that contain hapten. And during radiation and chemotherapy, blood monitoring should be carried out. In any case, constant consultations with your doctor and, if possible, regular blood checks are necessary. And, naturally, a healthy lifestyle, giving up bad habits, smoking, and alcohol are very important. Be healthy!