Author's rating
Author of the article
Green Elena Stanislavovna
Otolaryngologist of the second category
Articles written
665
about the author
Croup or stenosing laryngotracheobronchitis is a syndrome that occurs against the background of an acute infectious disease. The pathology affects the respiratory tract and without timely treatment can be fatal. Children are the most vulnerable, since their anatomical structure of the respiratory organs is somewhat different from the anatomy of adolescents and adults.
Causes
Croup in children develops against the background of infectious and inflammatory diseases accompanied by damage to the mucous membrane of the pharynx and trachea, for example, with influenza, adenovirus infection, measles, scarlet fever, chicken pox, diphtheria.
True croup develops as a result of swelling of the vocal folds (cords). The only example of this pathology is diphtheria stenotic laryngitis.
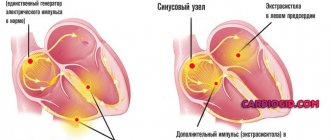
Obstruction of the respiratory tract during croup develops gradually, in stages and is associated with the direct effect on the mucous membrane of infectious agents and their waste products. Its final stage is asphyxia.
The pathological mechanism of development of croup in children is based on the following processes:
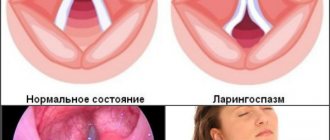
- reflex spasm of the muscles that narrow the larynx (constrictors);
- swelling of the inflamed mucous membrane of the larynx;
- hypersecretion of viscous thick mucus.
Obstruction of the respiratory tract that occurs with croup in children makes it difficult to breathe, resulting in an insufficient amount of oxygen entering the lungs for normal breathing. In turn, this leads to hypoxia – oxygen starvation of all organs and tissues of the body.
The general condition of children with croup directly depends on the severity of obstruction. In the initial stages, compensation for the resulting difficulty in breathing is carried out due to more intense work of the respiratory muscles. A further decrease in the lumen of the larynx is accompanied by a compensatory breakdown and the appearance of paradoxical breathing, in which the chest expands on exhalation and narrows on inhalation. The final stage of croup in children is asphyxia, which leads to death.
Symptoms of croup
The child has a characteristic barking cough and whistling sounds when entering and exhaling air. When coughing, the face acquires a reddish tint from the tension that the patient experiences when coughing and expectorating accumulated bacterial mucus. It is worth paying attention to the complexion; if the color is paler than usual, and the lips have a bluish tint, this means that the child is not only having difficulty breathing, but the body is not receiving the required amount of oxygen. With such indicators, immediate hospitalization of the child in a specialized hospital is recommended. A high temperature may indicate a severe infectious croup, such as diphtheria or epiglotitis. How quickly a child gets into the hands of doctors will determine his health, and sometimes his life.
Various pathologies of the upper respiratory tract and, as a consequence, narrowing of the walls of the lumen of the larynx lead to breathing problems. The air flow increases, so-called shortness of breath appears, which is accompanied by retraction of the jugular fossa and intercostal spaces. The pectoral muscles participate incorrectly in the respiratory process: when inhaling, the chest decreases, and when exhaling, it expands. Too active breathing leads to drying of the mucous membrane and the formation of a crust. Thus, an even greater narrowing of the lumen of the larynx appears, breathing is extremely difficult, and a characteristic whistle is heard. With abundant accumulation of mucus in the lumen of the larynx, the vocal cords wheeze and the voice is hoarse. The variability of breathing sounds indicates the dominance of spastic components of obstruction. A decrease in the intensity of breathing noise may indicate worsening stenosis.
Kinds
Croup in children, depending on the level of damage to the larynx, is divided into true and false. True croup develops as a result of swelling of the vocal folds (cords). The only example of this pathology is diphtheria stenotic laryngitis. With false croup in children, inflammatory swelling of the mucous membrane of the subglottic (subglottic) area of the larynx of non-diphtheria etiology is observed.
According to the etiology of the underlying disease, false croup in children is divided into the following types:
- viral;
- bacterial;
- fungal;
- chlamydial;
- mycoplasma
With timely initiation of treatment for croup in children, the prognosis is favorable, the disease ends in recovery.
According to the severity of obstruction, the following degrees of croup in children are distinguished:
- Compensated stenosis.
- Subcompensated (incomplete compensation) stenosis.
- Decompensated (uncompensated) stenosis.
- Terminal phase (asphyxia).
According to the nature of the clinical course of croup in children, it can be uncomplicated or complicated. Complicated is characterized by the addition of a secondary bacterial infection.
Diphtheria, or true croup, according to the degree of prevalence of the inflammatory process, in turn, is divided into non-extended (limited to the vocal cords) and widespread (descending) croup, in which the infectious process affects the trachea and bronchi.
Signs of croup in children
The clinical picture of croup in children includes the following symptoms:
- Noisy breathing (stridor). It is observed in croup of any etiology. The sound accompaniment of the act of breathing is associated with the vibration of the vocal cords, arytenoid cartilages and epiglottis. As laryngeal stenosis increases, the sonority of respiratory sounds decreases, which is associated with a decrease in tidal volume.
- Dyspnea. This is a mandatory symptom of croup in children. With subcompensated stenotic laryngitis, shortness of breath is inspiratory in nature, that is, the child experiences difficulty at the moment of inhalation. The transition of the disease to the decompensated stage is characterized by the appearance of mixed inspiratory-expiratory shortness of breath (both inhalation and exhalation are difficult). Increased body temperature and rapid breathing during croup in children are accompanied by significant loss of fluid with the development of respiratory exicosis.
- Dysphonia (change in voice). The development of this symptom of croup in children is associated with inflammatory changes in the vocal cords. With true croup, hoarseness of the voice gradually increases until it completely loses its sonority (aphonia). With false croup, aphonia never occurs.
- Barking rough cough. Its occurrence is explained by incomplete opening of the glottis against the background of spasm. Moreover, the stronger the swelling, the quieter the cough.
Croup in children can be complicated by the development of sinusitis, conjunctivitis, otitis media, pneumonia, bronchitis, and meningitis.
Complications
If you notice the disease in time and consult a doctor, neither of the two types of disease poses a threat to the life and health of the patient. If you ignore the symptoms and do not provide help for croup, there is a serious threat of death or other negative consequences. For diphtheria croup:
- cell damage from diphtheria toxin;
- disruption of the nervous system;
- peripheral paralysis of the vocal cords, limbs and airways;
- myocarditis;
- pneumonia;
- nephrotic syndrome;
- thrombosis;
- embolism;
- cerebral edema;
- renal, cardiovascular or respiratory failure;
- asphyxia.
For false croup:
- development of fibrinous-purulent films in the larynx;
- tracheobronchitis;
- pneumonia,
- asphyxia.
In most cases, croup stops at the first or second stage and does not progress further. Symptoms may persist for a day or two, but subsequently resolve on their own and usually do not affect health. If laryngeal stenosis continues to develop, immediate hospitalization is necessary, since the most severe consequence of croup is suffocation and death.
Diagnostics
Diagnosis of croup in children does not cause any difficulties and is carried out by a pediatrician or otolaryngologist based on the characteristic clinical picture of the disease, medical history, physical examination and laryngoscopy. If necessary, the child is consulted by an infectious disease specialist (diphtheria croup), a phthisiatrician (larynx tuberculosis), and a pulmonologist (bronchopulmonary complications).
When auscultating the lungs in children with croup, whistling dry rales are heard. The worsening of the disease is accompanied by the appearance of moist rales of various sizes.
When performing laryngoscopy, the degree of stenosis of the larynx, the extent of the pathological process, and the presence or absence of fibrinous films are determined.
To verify the pathogen, laboratory diagnostic methods are used: bacteriological culture and microscopy of throat swabs, serological tests (RIF, ELISA, PCR). In order to determine the severity of hypoxia, the acid-base state of the blood and its gas composition are determined.
If complications are suspected, lumbar puncture, radiography of the paranasal sinuses and lungs, rhinoscopy, otoscopy, and pharyngoscopy are prescribed.
Croup in children requires differential diagnosis with the following diseases:
- laryngeal tumors;
- bronchial asthma;
- epiglotitis;
- retropharyngeal abscess;
- foreign body of the larynx;
- whooping cough;
- congenital stridor.
Differential diagnosis of diphtheria croup and croup of other etiologies:
| Sign | True diphtheria croup | False croup |
| Voice | Increasing hoarseness of voice, turning into persistent aphonia | Hoarseness is inconsistent, there is no aphonia |
| Cough | Dry, rough, barking, dull, losing sonority, up to complete aphonia | Rough, barking, without losing sonority |
| Raids | Dirty white, difficult to remove, leaving a bleeding surface after plaque removal | Superficial, easy to remove |
| Cervical lymph nodes | Enlarged, swollen on both sides, slightly painful, swelling of the tissue around the nodes | Enlarged, very painful, no swelling. Individual lymph nodes are palpated |
| Development of stenosis | Laryngeal stenosis develops gradually, initially noisy breathing, turning into an attack of suffocation. Doesn't go away on its own | Stenosis occurs suddenly, often at night. The inhalation is loud and can be heard from a distance. Sometimes stenosis resolves spontaneously |
Differential diagnosis of true and false croup in children
The first symptoms of both true and false croup in children appear 2-3 days from the onset of the underlying disease. The clinical picture of true croup in children is characterized by a gradual increase in respiratory disorders.
Children with compensated forms of croup are subject to hospitalization in the department of acute respiratory infectious diseases of an infectious diseases hospital.
During the course of the disease, several stages are clearly visible:
- Dysphonic. There is hoarseness of the voice, there are no signs of obstruction.
- Stenotic. Against the background of increasing obstruction of the larynx, the child develops breathing difficulties and signs of hypoxia appear.
- Asphyxial. Almost complete obstruction of the larynx occurs. Severe hypoxia causes the development of hypoxic coma and death.
With false croup in children, the attack occurs suddenly and mainly at night. During the day, the condition of patients changes significantly.
With true croup, the vocal cords themselves swell in children, and therefore the sonority of the voice gradually decreases until complete aphonia (silent crying, screaming). Although false croup is accompanied by hoarseness of the voice, aphonia never develops with it. When crying and screaming in children with false croup, the sonority of the voice is preserved.
With true croup in children, laryngoscopy reveals swelling and hyperemia of the laryngeal mucosa, a decrease in its lumen, and the presence of diphtheria films. Diphtheria plaques are difficult to remove, with the formation of small ulcers underneath. The observed laryngoscopic picture with false croup is different. It is characterized by:
- redness and swelling of the mucous membrane;
- accumulation of thick sputum;
- laryngeal stenosis;
- easily removed plaque.
A bacteriological examination of a throat smear allows a final differential diagnosis between false and true croup in children. When diphtheria bacilli are isolated from the test material, the diagnosis of true croup is beyond doubt.
Clinical manifestations and diagnosis
Typical wedge manifestations of diphtheria K. are a hoarse, sometimes aphonic voice, a rough barking cough and stenosis of the respiratory tract (noisy breathing, retraction of the intercostal spaces of the chest, tension of the auxiliary respiratory muscles).
Depending on the severity, stenosis of degrees I, II and III is distinguished. During K. in diphtheria, three periods or stages are distinguished: the first is catarrhal, or the stage of croupous cough, the second is stenosis, and the third is asphyxia. There are no sharp boundaries between the stages; one passes into the other gradually and imperceptibly. The duration of the stages is also not strictly defined. For more details wedge, picture of diphtheria K. - see Diphtheria.
The greatest difficulties for diagnosis are presented by K. in influenza and acute respiratory viral diseases, which is one of the frequent and often initial manifestations of the disease; in some cases, K.'s syndrome is associated with influenza or acute respiratory disease several days after the onset of the disease. With these diseases, K.'s syndrome usually manifests itself suddenly (unlike diphtheria K., in which, as a rule, it develops gradually), and begins more often at night. The child was healthy in the evening before going to bed or had a slight runny nose; at night he suddenly wakes up from a coughing fit, he immediately has difficulty breathing; he is frightened, rushes about in bed, and cyanosis of the nasolabial triangle quickly appears. It is important to note that the voice in this case can be hoarse or hoarse, but during a cry ringing notes are almost always heard, in contrast to diphtheria K., in which the voice initially becomes hoarse, and by the time the stenosis develops, as a rule, aphonic (after with the exception of rare cases when the films are located in the subglottic space). The cough with influenza and acute respiratory diseases is initially dry, but very quickly, by the end of the first day, it becomes moist, which usually does not happen with diphtheria K.
K.'s course with parainfluenza and adenoviral infection is usually milder than with influenza; acutely developed stenosis quickly weakens or completely disappears a few hours after applying thermal procedures (hot general and foot baths, warm drinks, heating pads for the feet, mustard plasters on the larynx area). In some cases, the phenomena of stenosis may be repeated the next night, but they pass just as safely as the first time.
K. with influenza is often more severe; acutely developed stenosis can progress quickly, within several hours. In some cases, the course of stenosis during influenza has a wave-like character - it sometimes increases or decreases even within a day, lasting from 7 to 10 days. The severity and duration of influenza K. depend not only on the severity of the necrotic process in the larynx, trachea and bronchi, but also on the often associated pneumonia. Establishing the etiology of an acute respiratory disease, against the background of which K.'s syndrome arose, is possible only by taking into account all the wedges, manifestations of the disease, as well as the results of virusol, and serol, studies on the respiratory group of viruses (see Virological studies, Serological studies).
Measles K. sometimes poses no less difficulties for diagnosis. Measles K. can be early if it develops during the prodrome of measles (see); in this case, severe stenosis is usually not observed and by the time the rash appears, it has weakened significantly. Late measles K., which appears during the period of pigmentation, is more severe. At the same time, changes in the larynx and trachea are often necrotic in nature and the course of stenosis is as long and often wave-like as with influenza K. Diagnosis of late measles K. in previous years was especially difficult because during the period of pigmentation of the rash due to the weakening of immunobiol , the state of the body could be associated with diphtheria infection. This should be kept in mind now. Although diphtheria in the second half of the 20th century. It is extremely rare; contact with diphtheria bacteria is possible.
Treatment of croup in children
Children with compensated forms of croup are subject to hospitalization in the department of acute respiratory infectious diseases of an infectious diseases hospital. In sub- and decompensated forms, treatment of children should be carried out in specialized emergency departments under the supervision of an otolaryngologist and resuscitator.
Prevention of true croup is based on mass vaccination of children against diphtheria in accordance with the national immunization calendar.
Treatment of croup in children is based on the following principles:
- children are placed in rooms with an air temperature of no more than 18 °C;
- for true croup, anti-diphtheria serum is prescribed intravenously or intramuscularly;
- antibiotic therapy - indicated for children with true croup or false croup complicated by a secondary bacterial infection;
- inhalation therapy - carried out only for children with a preserved cough reflex;
- prescription of a short course of glucocorticosteroids (duration 2-3 days);
- antiallergic treatment - antihistamines should be prescribed with extreme caution to children with a pronounced hypersecretory component of inflammation);
- detoxification therapy (intravenous administration of solutions of electrolytes, glucose) – aimed at reducing the severity of intoxication syndrome, correcting water and electrolyte disorders caused by respiratory exicosis;
- for a dry non-productive cough, antitussive drugs are prescribed, and for a wet cough, mucolytics are prescribed;
- prescribing antispasmodics to eliminate reflex spasm of the pharyngeal constrictor muscles;
- sedative therapy for severe agitation of the child;
- when signs of hypoxia appear, oxygen therapy is performed (inhalation of humidified oxygen through a face mask or nasal catheters, placing the child in an oxygen tent);
- If conservative treatment of croup in children accompanied by severe respiratory failure is ineffective, tracheal intubation or tracheostomy is performed.
Source: 17nov.ru
Prevention
Prevention of true croup is based on mass vaccination of children against diphtheria in accordance with the national immunization calendar.
Specific prevention of false croup has not been developed. To reduce the risk of its occurrence it is necessary:
- avoid contact of children with people who have signs of acute infectious and inflammatory diseases of the respiratory tract;
- strengthen the body's defenses (following a daily routine, proper nutrition, regular walks in the fresh air, hardening procedures);
- vaccinate against influenza, measles, mumps, and chickenpox.
Video from YouTube on the topic of the article: