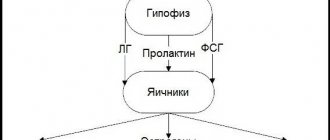
Prolactinoma, a pituitary tumor, is a benign tumor (called an adenoma) of the pituitary gland. The pituitary gland is a part of the brain that regulates the activity of various endocrine glands - the thyroid gland, adrenal glands, ovaries and testicles. The pituitary gland produces a number of hormones, including prolactin, follicle-stimulating hormone (FSH) and luteinizing hormone (LH), adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH). With the help of these hormones, the pituitary gland controls individual endocrine glands: ACTH regulates the functioning of the adrenal glands, TSH regulates the functioning of the thyroid gland, FSH and LH regulate the functioning of the ovaries.
Prolactinoma
is one of the most common types of pituitary tumors. The results of routine autopsies performed after a person's death have shown that about a quarter (25%) of the population have small tumors of the pituitary gland.
Prolactin-secreting adenomas (prolactinomas) are the most common hormonally active pituitary tumors. Prolactinoma produces excessive amounts of the hormone prolactin. Prolactin is a natural hormone that contributes to the normal process of milk production in a woman. Prolactin stimulates breast tissue to enlarge during pregnancy. After the baby is born, the mother's prolactin levels drop until she begins to breastfeed. Every time a baby latch onto the breast, prolactin levels rise and promote milk production. Normally, prolactin, LH and FSH regulate sex life and reproduction. In women, they stimulate the formation of female sex hormones - estrogens and egg maturation, and also regulate the menstrual cycle. In men, these hormones stimulate the production of the male sex hormone, testosterone, as well as sperm motility.
Norm prolactin
It is noted that the amount of this hormone does not always reflect the strength of clinical manifestations. For example, women with severe hyperprolactinemia may have regular menstruation, good ability to conceive and bear a child, and a slight excess of the norm may be combined with serious and unpleasant symptoms.
This phenomenon is associated with the existence of 4 different forms of the hormone:
- "small" BPD
- "big" BPD
- macro-PRL
- glycosylated PRL
All of these forms have different effects on target organs, so their identification is extremely important. Microprolactin is considered the most active; it is the one that causes all external manifestations of hormonal imbalance. Large forms of this substance are bound and therefore almost inactive.
Outside of pregnancy, a woman’s normal level of the hormone prolactin does not exceed 20 ng/ml (600 µU/ml). A rise in level to 1000 µU/ml is considered mild and insignificant. If hyperprolactinemia is detected, a macroprolactin test is additionally prescribed. If its amount exceeds 60%, then bioactive PRL is only 40%, which may well be within the normal range. If macroprolactin is low (less than 40%), then the active hormone is still outside the normal range and requires further examination.
Prognosis for tumor
Microadenomas have the most favorable course. You can get rid of them even without surgery. After removal of medium-sized tumors, relapse occurs in a third of patients within 5 years. Large tumors significantly change the hormonal levels in the body, so even surgical treatment mainly relieves signs of brain compression.
The period during which clinical remission occurs with medications depends on the size and hormonal activity of prolactinoma. Treatment usually lasts for several years. If the patient stops it on his own, the tumor grows rapidly and may develop into a malignant neoplasm.
Prolactin during pregnancy
As the day of birth approaches, the amount of estrogen in the blood of the expectant mother increases. This, in turn, stimulates the synthesis of PRL, the level of which increases several times, which is the absolute norm. Therefore, for pregnant women, this test is not informative and is not taken.
Nature has created such a mechanism so that by the time a child is born, a woman’s mammary glands are ready to secrete milk. PRL increases to its maximum at 25 weeks and decreases slightly before birth. With the first breastfeeding, prolactin levels increase in response to nipple stimulation.
Diagnosis and indications for treatment
Diagnosis and treatment of prolactinoma is the same in both men and women. If health deteriorates, if a tumor of the pituitary gland is suspected, diagnosis is mandatory. Self-treatment, even with absolute confidence that there is a pituitary tumor, is unacceptable! Treatment should be prescribed only by a specialist, after a thorough diagnosis. The diagnostic procedure is as follows:
- Consultation with an endocrinologist, consultation with a gynecologist (for women), consultation with an andrologist (for men).
- Blood test for prolactin, blood test for the percentage of macroprolactin opening.
- Blood test for thyroid hormones, pituitary gonadotropic hormones, testosterone, estradiol (for women).
- Magnetic resonance imaging (MRI) in case of suspected pituitary tumor.
- Ultrasound examination (ultrasound) of the uterus and ovary (for women), prostate gland (for men).
- Consultation with an ophthalmologist to determine whether there is a macrotumor of the pituitary gland.
- Bone densitometry in cases of suspected osteoporosis.
Separately, it is necessary to clarify the analysis for prolactin. This is the most important test when making a diagnosis, so you need to prepare for it. It is important to know that women need to be tested for prolactin in the first phase of the menstrual cycle (on days 3-5)!
Blood is drawn from a vein; this must be done in the morning, on an empty stomach. The day before donating blood for prolactin, sexual contact, visiting a sauna or bathhouse, and drinking alcohol are strictly prohibited. A couple of hours before blood sampling, you must stop smoking. Women need to be extremely careful not to injure their breasts before having a blood test. It is also advisable to reschedule blood sampling for prolactin analysis after severe stress. Following these recommendations is important because any violation of the correct regimen may cause inaccurate test results.
As a rule, the result of a prolactin analysis will be ready in 5-6 days. Normal serum prolactin levels range from 110 to 550 mU/L in women and up to 400 mU/L in men. If these values are exceeded, we can talk about the presence of prolactinoma.
Hormone functions
Prolactin has many different effects on the female body. This is not surprising, because there are receptors for it in the mammary glands, ovaries, uterus, placenta, liver, eyes, lymphatic and immune cells, brain, kidneys, adrenal glands, intestines and pancreas.
Effects of BPD:
- Prepares the mammary glands for lactation
- Stimulates milk synthesis after childbirth
- In the second phase of the cycle, it supports the functioning of the corpus luteum, which produces progesterone.
- Takes part in the ovulation process
- Regulates the composition and volume of amniotic fluid
- Has immune properties
results
With systematic treatment with a high-quality drug in the correct dosage, normalization of impaired body functions occurs. For example, a large number of married couples who were unable to have children because one of the spouses had prolactinoma became happy parents after a course of treatment.
The serious disadvantages of this pathology include the forced long-term use of a prolactin-lowering drug, since after cessation of treatment, in 98% of patients the level of prolactin in the blood increases again. To maintain normal prolactin, the attending physician selects the optimal dosage of the drug. Most often, a quarter of a tablet per week (in one dose) is prescribed as a maintenance dosage.
Symptoms of hyperprolactinemia
- Menstrual irregularities (infrequent or absent periods)
- Infertility (due to lack of ovulation or shortening of the 2nd phase of the cycle)
- Galactorrhea (leakage of milk from the breast) – occurs in 70% of cases
- Headache, loss of vision (with large pituitary tumors)
- Decreased libido
- Acne, facial hair growth (in 20% of patients)
- Osteoporosis
- Obesity (in 40-60% of cases)
- Depression, insomnia (in 20% of cases of hyperprolactinemia)
- Memory loss
Prolactinoma: consequences and prognosis
The question is often asked: “What happens if prolactinoma is not treated?” Firstly, there will be a constantly elevated level of prolactin, which disrupts the functioning of the gonads and also negatively affects the entire body, we wrote about this in our other articles.
Secondly, the tumor can compress the surrounding delicate brain tissue and lead to dire consequences. For example, to blindness. Therefore, the prognosis for life without treatment is not comforting; the disease will progress.
If you start treatment or operate on a large tumor, the prognosis is more favorable. A person can completely get rid of the disease and live a normal life.
Reasons for increased prolactin levels
Physiological
| Pathological
| Taking medications
|
Physiological reasons
The amount of hormone in each individual woman varies throughout the day. It is known that during sleep the level of PRL increases, starting from 60-90 minutes. This occurs both during night rest and during daytime sleep, and after waking up the amount of the hormone drops sharply. A slight rise is also observed during physical activity, sexual intercourse, and also after eating protein foods. Stress reactions can also affect the hormone, especially when combined with physical stress (for example, fainting during a blood draw is a guarantee of an increase in PRL).
Pituitary gland diseases
Prolactinoma, a common tumor of the pituitary gland, is the most common cause of high levels of PRL in the blood. Depending on its size, it is called microprolactinoma (less than 1 cm) or macroprolactinoma (more than 1 cm). About a quarter of the world's population has undiagnosed pituitary microtumors, which do not cause significant symptoms and may simply be an incidental finding.
Most often, such adenoma is diagnosed in women aged 30-40 years. The female sex is characterized by the small size of the neoplasm. In addition to impairing reproductive function, the tumor can compress the visual pathways, leading to loss of vision, as well as cause headaches and impair quality of life. Therefore, with a proven adenoma (prolactin is higher than normal due to the microfraction, MRI shows a tumor), treatment with Dostinex or surgical removal is necessary (extremely rare). When planning a pregnancy, you need to take Dostinex for a year, then if you successfully try to conceive, stop the drug.
Other pituitary tumors
Any neoplasm that blocks the pathways between the pituitary gland and the hypothalamus can cause an increase in the concentration of PRL in the blood. Sometimes they are all combined under the term “pseudoprolactinoma,” although along with prolactin the amount of other hormones (GH, ACTH) also increases. Most of them have their own features on MRI and CT, but the number of PRL is much lower than in the case of true prolactinoma.
Primary hypothyroidism
The connection between decreased thyroid function and increased PRL in the blood has not yet been precisely explained. But almost half of patients with hypothyroidism have similar changes in tests. After starting replacement therapy, prolactin also returns to normal. We must not forget that hypothyroidism can easily coexist with brain tumors and other pathologies.
Polycystic ovary syndrome
The classic case of PCOS includes menstrual irregularities, ovarian cysts, and elevated androgen levels. But in 30-40% of cases, hyperprolactinemia is added to these signs. The reasons for this relationship are not precisely known. But for any suspicion of PCOS, it is necessary to take a test for prolactin and macroprolactin in order to prescribe the necessary treatment (see polycystic ovary syndrome).
Chest injuries
It is known that various surgical interventions can increase the PRL indicator for a period from a day (for abdominal surgery) to several months (for manipulations in the chest area). The same effect occurs with herpes zoster (Herpes zoster virus), which affects the skin of the upper body. This is due to increased nerve impulses from the damaged area to the brain. The closer the source of irritation is to the mammary glands, the more intense and durable these impulses are.
Idiopathic hyperprolactinemia
It happens that a moderate increase in the amount of the hormone in the blood (25-80 ng/ml) exists independently, without visible pathology of the hypothalamus and pituitary gland. Such cases are called idiopathic (causeless). Most people with this form of the syndrome have macroprolactinemia without needing treatment.
Hypothalamic diseases
The hypothalamus is one of the highest links in the endocrine system. Therefore, any disruption of its function leads to changes in the level of all hormones, including PRL. Hyperprolactinemia may result from a hypothalamic tumor, craniopharyngioma, glioma, inflammation in the brain, metastatic disease, and abnormal vascular development. A similar effect occurs with therapeutic irradiation of the brain.
Estrogen-producing tumors
Many neoplasms are capable of secreting hormones. In women, ovarian tumors often synthesize estrogen in large quantities. This leads to a natural increase in prolactin. Therefore, such changes in tests are a reason to examine the pelvic area with an ultrasound.
Taking medications
Sometimes prolactin in women is increased when taking certain medications: antipsychotics (haloperidol, aminazine), antiemetics (cerucal, moltilium), reserpine, levodopa, opiate substances (morphine), verapamil, hormonal contraceptives.
Causes of pituitary prolactinoma
Like most tumor diseases, pituitary adenoma occurs for reasons that are not fully understood. In some patients, excessive growth and activity of cells that form prolactin is observed in a genetically determined disease. It is called polyendocrine neoplasia.
Growth of pituitary adenoma
This means that the endocrine glands, due to a failure of regulation, go beyond the control of the hypothalamus and begin to intensively produce hormones. In such cases, the function of the parathyroid glands, pancreas, and pituitary gland increases. Multiple ulcerative defects are found in the digestive system. Isolated inheritance of a tendency to prolactinoma also occurs.
We recommend reading the article about pituitary insufficiency. From it you will learn about the causes and symptoms of pituitary insufficiency, types of hypopituitarism, as well as the diagnosis and treatment of pituitary insufficiency.
And here is more information about pituitary adenoma.
Reasons for decreased prolactin levels
- Pituitary infarction after childbirth
- Taking medications
Pituitary infarction (Sheehan syndrome)
During pregnancy, a woman's pituitary gland increases in size, but its blood supply does not improve. Therefore, massive blood loss or a drop in pressure during labor can lead to a heart attack of this important organ. As a result, pituitary cells die and there is a deficiency of hormones, including prolactin. In such patients, prolactin levels in tests are low, so breastfeeding is impossible. If the volume of the pituitary gland that has undergone necrosis is too large, then the woman will need replacement therapy.
Taking medications
Some medications and substances can reduce hormone secretion: dopamine, pyridoxine, diuretics, nicotine. The latter explains problems with breastfeeding when smoking, when prolactin is below normal.
Treatment of pituitary prolactinoma
This is practically the only pituitary adenoma that responds to drug therapy. Patients are prescribed Parlodel; it restores normal hormone levels in almost 90% of patients within a month. Dostinex is not inferior to it in effectiveness, but has fewer undesirable consequences during long-term treatment; it is enough to take it once every 7-10 days.
These medications lead to a reduction in prolactinoma and cessation of its hormonal activity. Patients' vision is restored, and small tumors may disappear. The medications normalize menstruation, sexual function, and possible pregnancy. Large tumors require MRI monitoring throughout the course of therapy.
If there is no positive dynamics in the size of the prolactinoma and its synthesis of prolactin, vision declines, then removal of the adenoma is indicated. The operation can be performed through the nasal passages or by craniotomy.
Watch the video about the diagnosis and treatment of pituitary adenoma (prolatinoma):
There are cases when radiation therapy is prescribed; it makes it possible not to use medications if there are contraindications, individual intolerance, or lack of results.
The effect of radiation becomes fully apparent after 2-3 years and lasts up to 5 years . Therefore, this method is not recommended for women who are planning to have a child. A complication of radiation therapy is pituitary failure. To correct it, Hydrocortisone, Euthyrox, Methyltestosterone for men and Divigel for women are used.
Additional examination
If a blood test shows three times that the amount of PRL is not normal, then additional tests are usually performed:
- History of medication use
- Assessment of thyroid function (TSH, free T4)
- CT, MRI of the pituitary gland and hypothalamus
- Ultrasound of the pelvic organs
- Assessment of liver and kidney function (biochemical blood test, ultrasound)
- Hormonal profile (FSH, androgens, estradiol)
Any changes in a woman’s hormonal profile are indications for further examination. If there are deviations only in the numbers on the form, and there are no symptoms at all, then treatment is most likely not required.
Author:
Evtushenko Anna Aleksandrovna obstetrician-gynecologist
What should prolactin be for a pituitary adenoma?
If the cells of the pituitary gland begin to increase in size, and a prolactinoma is formed, which intensively produces prolactin, then its concentration in the blood increases (hyperprolactinemia) by more than 10 times. If the values obtained do not exceed 100 ng/ml, then other diseases that lead to an increase in the hormone must be excluded.
How to exclude an artificial increase in prolactin when diagnosing pituitary adenoma.
It should be borne in mind that an increase in prolactin levels can be influenced by external and internal factors, therefore, to obtain a reliable result when examining for the detection of pituitary adenoma, it is recommended:
- donate blood 3 times with an interval of 2-4 days;
- undergo analysis in case of acute inflammatory process, infection, injury, especially in the chest area;
- if an increase is detected, take a test for the level of microprolactin (an inactive form of the hormone); if it is higher than normal, then treatment will not be required;
- after consultation with a doctor, stop taking hormonal medications, vitamins and dietary supplements 15 days in advance;
- a day before, abstain from drinking alcohol, sports training, sexual intercourse, stimulation of the mammary gland area (chest massage, physiotherapy), visiting the sauna, solarium, or staying on the beach is prohibited;
- reduce the overall level of stress - practice long walks, relaxation sessions, take medicinal soothing teas or prescribed sedatives, avoid emotional stress immediately before the examination.