Anemia
or
“anemia”
- a decrease in the concentration of hemoglobin in the blood below established standards, most often, with a simultaneous decrease in the total volume of red blood cells (red blood cells that carry oxygen). Anemia, as a secondary symptom, can accompany various diseases, causing the development of oxygen starvation of tissues. The patient experiences chronic fatigue and weakness, constant drowsiness and loss of strength, dizziness and shortness of breath.
Content
- 1 Classification
- 2 Etiology 2.1 Blood loss of various origins
- 2.2 Unbalanced diet
- 2.3 Impaired absorption of iron
- 4.1 Prelatent iron deficiency in the body
- 5.1 Clinical blood test
Classification of anemia by color index
The color index determines the level of saturation of red blood cells with hemoglobin. It is calculated during a laboratory blood test using a special formula. Depending on the results obtained, there are:
Etiology
The cause of iron deficiency is an imbalance in its balance towards the predominance of iron consumption over intake, observed in various physiological conditions or diseases:
- blood loss of various origins;
- increased need for iron;
- impaired absorption of iron;
- congenital iron deficiency;
- impaired iron transport due to transferrin deficiency[1].
Blood loss of various origins
Increased consumption of iron, causing the development of hyposideropenia, is most often associated with blood loss or with its increased use in certain physiological conditions (pregnancy, periods of rapid growth). In adults, iron deficiency usually develops due to blood loss. Most often, constant small blood losses and chronic hidden bleeding (5 - 10 ml/day) lead to a negative iron balance. Sometimes iron deficiency can develop after a single massive loss of blood that exceeds the iron reserves in the body, as well as due to repeated significant bleeding, after which the iron reserves do not have time to recover.
Various types of blood loss leading to the development of posthemorrhagic iron deficiency anemia are distributed in frequency as follows: in the first place are uterine bleeding, then bleeding from the digestive canal. Rarely, sideropenia can develop after repeated nasal, pulmonary, renal, trauma bleeding, bleeding after tooth extraction and other types of blood loss. In some cases, iron deficiency, especially in women, can be caused by frequent blood donations from donors, therapeutic bloodletting for hypertension and erythremia. There are iron deficiency anemias that develop as a result of bleeding into closed cavities with a lack of subsequent reutilization of iron (pulmonary hemosiderosis, ectopic endometriosis, glomic tumors).
According to statistics, 20 - 30% of women of childbearing age have a hidden iron deficiency, and 8 - 10% have iron deficiency anemia. The main cause of hyposiderosis in women, in addition to pregnancy, is pathological menstruation and uterine bleeding. Polymenorrhea can cause a decrease in iron reserves in the body and the development of hidden iron deficiency, and then iron deficiency anemia. Uterine bleeding increases the volume of blood loss in women to the greatest extent and contributes to the occurrence of iron deficiency conditions. There is an opinion that uterine fibroids, even in the absence of menstrual bleeding, can lead to the development of iron deficiency. But more often the cause of anemia with fibroids is increased blood loss.
The second most common factor causing the development of posthemorrhagic iron deficiency anemia is blood loss from the digestive canal, which is often hidden and difficult to diagnose. In men, this is generally the main cause of sideropenia. Such blood loss can be caused by diseases of the digestive system and diseases of other organs. Iron imbalances can be accompanied by repeated acute erosive or hemorrhagic esophagitis and gastritis, peptic ulcer of the stomach and duodenum with repeated bleeding, chronic infectious and inflammatory diseases of the digestive canal. With giant hypertrophic gastritis (Menetrier's disease) and polypous gastritis, the mucous membrane is easily vulnerable and often bleeds. A common cause of hidden, difficult to diagnose blood loss is a hiatal hernia, varicose veins of the esophagus and rectum with portal hypertension, hemorrhoids, diverticula of the esophagus, stomach, intestines, Meckel's duct, tumors. Pulmonary hemorrhage is a rare cause of iron deficiency. Bleeding from the kidneys and urinary tract can sometimes lead to the development of iron deficiency. Hypernephroma is very often accompanied by hematuria.
In some cases, blood loss of various locations, which is the cause of iron deficiency anemia, is associated with hematological diseases (coagulopathies, thrombocytopenias and thrombocytopathies), as well as with vascular damage due to vasculitis, collagenosis, Randu-Weber-Osler disease, hematomas.
Sometimes iron deficiency anemia, caused by blood loss, develops in newborns and infants. Children are much more sensitive to blood loss than adults. In newborns, blood loss may be a consequence of bleeding observed during placenta previa or its damage during cesarean section. Other difficult-to-diagnose causes of blood loss during the neonatal period and infancy: bleeding from the digestive canal due to infectious diseases of the intestines, intussusception, and from Meckel’s diverticulum. Much less often, iron deficiency can occur when there is insufficient intake of iron into the body.
Unbalanced diet
Iron deficiency of nutritional origin can develop in children and adults with insufficient iron content in the diet, which is observed with chronic malnutrition and starvation, with dietary restriction for therapeutic purposes, with monotonous food with a predominant content of fats and sugars. Children may experience insufficient intake of iron from the mother's body as a result of iron deficiency anemia during pregnancy, premature birth, multiple births and prematurity, premature ligation of the umbilical cord before the pulsation stops.
Impaired absorption of iron
For a long time, the main cause of iron deficiency was considered to be the lack of hydrochloric acid in gastric juice. Accordingly, gastrogenic or achlorhydric iron deficiency anemia was distinguished. It has now been established that achilia can only have an additional significance in disrupting the absorption of iron in conditions of increased need for it in the body. Atrophic gastritis with achylia occurs due to iron deficiency, caused by a decrease in enzyme activity and cellular respiration in the gastric mucosa.
Inflammatory, cicatricial or atrophic processes in the small intestine and resection of the small intestine can lead to impaired iron absorption. There are a number of physiological conditions in which the need for iron sharply increases. These include pregnancy and lactation, as well as periods of increased growth in children. During pregnancy, iron consumption increases sharply for the needs of the fetus and placenta, blood loss during childbirth and lactation. The iron balance during this period is on the verge of deficiency, and various factors that reduce iron intake or increase iron consumption can lead to the development of iron deficiency anemia.
There are two periods in a child’s life when there is an increased need for iron. The first period is the first - second year of life, when the child grows quickly. The second period is the period of puberty, when rapid development of the body begins again; girls experience additional iron consumption due to menstrual bleeding.
Iron deficiency anemia sometimes, especially in infancy and old age, develops with infectious and inflammatory diseases, burns, tumors, due to impaired iron metabolism while its total amount is preserved.
What it is?
According to WHO (World Health Organization), more than 2 billion people on the planet have iron deficiency in their bodies. Iron is part of most enzymes and is the main component of hemoglobin. Without it, the hematopoietic process and respiration, various vital oxidative and reducing reactions, are impossible.
The development of iron deficiency and subsequent anemia may be due to various mechanisms. Most often, iron deficiency anemia is caused by chronic blood loss:
- heavy menstruation,
- dysfunctional uterine bleeding;
- gastrointestinal bleeding from erosions of the gastric and intestinal mucosa,
- gastroduodenal ulcers,
- hemorrhoids,
- anal fissures, etc.
The main causes of deficiency in the body are:
- unbalanced diet (malnutrition can lead to the development of iron deficiency anemia in both children and adults);
- lack of vitamins;
- increased iron requirements;
- diseases of the gastrointestinal tract.
The cause of congenital iron deficiency in the body can be:
- severe iron deficiency anemia in the mother;
- multiple pregnancy;
- prematurity.
During long-term chronic infections (tuberculosis, sepsis, brucellosis), iron molecules are captured by immune cells, and a deficiency is detected in the blood.
Older people more often suffer from a lack of iron in the body, and this is understandable: there is a natural degradation of hematopoietic functions, in addition, various diseases cause blood loss - for example, infections and inflammations, ulcers and erosions.
Pathogenesis
Iron deficiency anemia is associated with the physiological role of iron in the body and its participation in the processes of tissue respiration. It is part of heme, a compound that can reversibly bind oxygen. Heme is the prosthetic part of the hemoglobin and myoglobin molecules. Ferritin and hemosiderin are of primary importance in the deposition of iron in the body. The transport of iron in the body is carried out by the protein transferrin (siderophilin).
The body can only to a small extent regulate the intake of iron from food and does not control its expenditure. With a negative balance of iron metabolism, iron is first consumed from the depot (latent iron deficiency), then tissue iron deficiency occurs, manifested by impaired enzymatic activity and respiratory function in tissues, and only later does iron deficiency anemia develop.
Iron supplements
Iron deficiency can be treated with iron supplements
Medicines that replenish iron deficiency are presented in the table:
| Name | Release form |
| Hemofer | Solution |
| Aktiferon | Syrup, capsules |
| Tardiferon | Pills |
| Hemophere prolongatum | Dragee |
| Sorbifer Durules | Pills |
| Maltofer (Ferrum-Lek) | Syrup, drops, solution, chewable tablets |
| Gyno-Tardiferon | Pills |
| Fenotek | Capsules |
| Fenyuls | Capsules |
| Ferro foil | Capsules |
| Venofer | Solution |
| Ferinject | Solution |
Clinical picture and stages of disease development
IDA is the last stage of iron deficiency in the body. There are no clinical signs of iron deficiency in the initial stages, and diagnosis of the preclinical stages of iron deficiency has become possible only thanks to the development of laboratory diagnostic methods. Depending on the severity of iron deficiency in the body, three stages are distinguished:
- prelatent iron deficiency in the body;
- latent iron deficiency in the body;
- Iron-deficiency anemia.
Prelatent iron deficiency in the body
At this stage, depot depletion occurs in the body. The main form of iron storage is ferritin, a water-soluble glycoprotein complex found in macrophages of the liver, spleen, bone marrow, erythrocytes and blood serum. A laboratory sign of depletion of iron stores in the body is a decrease in serum ferritin levels. At the same time, the level of serum iron remains within normal values. There are no clinical signs at this stage, and the diagnosis can only be made based on determination of serum ferritin levels.
Latent iron deficiency in the body
If adequate replenishment of iron deficiency does not occur at the first stage, the second stage of iron deficiency occurs - latent iron deficiency. At this stage, as a result of disruption of the supply of the required amount of metal to the tissue, there is a decrease in the activity of tissue enzymes (cytochromes, catalase, succinate dehydrogenase, etc.), which is manifested by the development of sideropenic syndrome. Clinical manifestations of sideropenic syndrome include taste perversion, addiction to spicy, salty, spicy foods, muscle weakness, degenerative changes in the skin and appendages, etc.
At the stage of latent iron deficiency in the body, changes in laboratory parameters are more pronounced. Not only depletion of iron stores in the depot is recorded - a decrease in serum ferritin concentration, but also a decrease in iron content in serum and transport proteins.
Serum iron is an important laboratory indicator, on the basis of which it is possible to carry out differential diagnosis of anemia and determine treatment tactics. But it should be remembered that it is impossible to draw conclusions about the iron content in the body only from the level of serum iron. Firstly, because the level of serum iron is subject to significant fluctuations during the day, depending on gender, age, etc. Secondly, hypochromic anemia can have different etiologies and pathogenetic mechanisms of development, and determining only the level of serum iron does not answer the questions pathogenesis. Thus, if during anemia there is a decrease in serum iron levels along with a decrease in serum ferritin, this indicates an iron deficiency etiology of anemia, and the main treatment tactic is to eliminate the causes of iron loss and replenish its deficiency. In another case, a reduced level of serum iron is combined with a normal level of ferritin. This occurs in iron redistribution anemia, in which the development of hypochromic anemia is associated with a disruption in the process of iron release from the depot. The treatment tactics for redistribution anemia will be completely different - prescribing iron supplements for this anemia is not only inappropriate, but can cause harm to the patient.
Total iron-binding capacity of serum (TIBC) is a laboratory test that makes it possible to determine the degree of so-called “Fe-starvation” of serum. When determining the TLC, a certain amount of iron is added to the test serum. Some of the added iron is bound to carrier proteins in the serum, and the iron that is not bound to proteins is removed from the serum and its amount is determined. In iron deficiency anemia, the patient's serum binds more iron than normal—an increase in the life-saving value is recorded.
Transferrin saturation with iron, %. The main iron transport protein in blood serum is transferrin. Transferrin synthesis occurs in the liver. One transferrin molecule can bind two iron atoms. Normally, transferrin saturation with iron is about 30%. At the stage of latent iron deficiency in the body, transferrin saturation with iron decreases (less than 20%).
Iron-deficiency anemia
The iron deficiency state depends on the degree of iron deficiency and the rate of its development and includes signs of anemia and tissue iron deficiency (sideropenia). The phenomena of tissue iron deficiency are absent only in some iron deficiency anemias caused by impaired iron utilization, when the depots are overfilled with iron. Thus, iron deficiency anemia goes through two periods in its course: the period of hidden iron deficiency and the period of obvious anemia caused by iron deficiency. During the period of latent iron deficiency, many subjective complaints and clinical signs characteristic of iron deficiency anemia appear, only less pronounced. Patients note general weakness, malaise, and decreased performance. Already during this period, distortion of taste, dryness and tingling of the tongue, difficulty swallowing with the sensation of a foreign body in the throat (Plummer-Vinson syndrome), palpitations, and shortness of breath may be observed.
An objective examination of patients reveals “minor symptoms of iron deficiency”: atrophy of the tongue papillae, cheilitis (“seizures”), dry skin and hair, brittle nails, burning and itching of the vulva. All these signs of impaired trophism of epithelial tissues are associated with tissue sideropenia and hypoxia.
Hidden iron deficiency may be the only sign of iron deficiency. Such cases include often pronounced sideropenia, which develops over a long period of time in women of mature age due to repeated pregnancies, childbirth and abortions, in female donors, in persons of both sexes during periods of increased growth. In most patients with continued iron deficiency after the depletion of its tissue reserves, iron deficiency anemia develops, which is a sign of severe iron deficiency in the body. Changes in the function of various organs and systems in iron deficiency anemia are not so much a consequence of anemia as of tissue iron deficiency. Proof of this is the discrepancy between the severity of the clinical manifestations of the disease and the degree of anemia and their appearance already at the stage of latent iron deficiency.
Patients with iron deficiency anemia report general weakness, fatigue, difficulty concentrating, and sometimes drowsiness. Headache after overwork and dizziness appear. Severe anemia may cause fainting. These complaints, as a rule, depend not on the degree of anemia, but on the duration of the disease and the age of the patients.
Iron deficiency anemia is characterized by changes in the skin, nails and hair. The skin is usually pale, sometimes with a slight greenish tint (chlorosis) and with an easy blush on the cheeks, it becomes dry, flabby, peels, and cracks easily form. Hair loses its shine, turns grey, thins, breaks easily, thins and turns gray early. Changes in nails are specific: they become thin, matte, flattened, easily peel and break, and striations appear. With pronounced changes, the nails acquire a concave, spoon-shaped shape (koilonychia).
Classification of anemia by severity
The severity of anemia, determined by blood parameters depending on the age and gender of the patient, is conventionally divided into mild, moderate and severe. The mild form is characterized by a decrease in hemoglobin concentration to 90 g/l (the patient may experience general weakness and increased fatigue). The average degree is determined by the range from 70 to 90 g/l (patients complain of shortness of breath, tachycardia, headache, sleep disturbance, tinnitus, loss of appetite), and severe - below the limit of 70 g/l (the main danger of this condition is the development heart failure).
Diagnostics
Clinical blood test
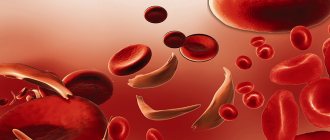
In a general blood test for IDA, a decrease in the level of hemoglobin and red blood cells will be recorded. Moderate erythrocytopenia can occur with Hb <98 g/l, but a decrease in red blood cells <2·1012/l is not typical for IDA. In case of IDA, changes in the morphological characteristics of erythrocytes and erythrocyte indices, which quantitatively reflect the morphological characteristics of erythrocytes, will be recorded.
Morphological characteristics of red blood cells The size of red blood cells is normal, increased (macrocytosis) or decreased (microcytosis). IDA is characterized by the presence of microcytosis. Anisocytosis is differences in the size of red blood cells in the same person. IDA is characterized by pronounced anisocytosis. Poikilocytosis is the presence of red blood cells of different shapes in the blood of the same person. In IDA, there may be pronounced poikilocytosis. The color index of erythrocyte cells (CR) depends on the hemoglobin content in them. The following options for staining red blood cells are possible:
- normochromic erythrocytes (CP = 0.85-1.05) - normal hemoglobin content in erythrocytes. Red blood cells in a blood smear have a uniform pink color of moderate intensity with a slight clearing in the center;
- hypochromic erythrocytes (CP<0.85) - the hemoglobin content in the erythrocyte is reduced. In a blood smear, such red blood cells have a pale pink color with a sharp clearing in the center. For IDA, hypochromia of erythrocytes is characteristic and is often combined with microcytosis;
- hyperchromic erythrocytes (CP>1.05) - the hemoglobin content in erythrocytes is increased. In a blood smear, these red blood cells have a more intense color, the lumen in the center is significantly reduced or absent. Hyperchromia is associated with an increase in red blood cell thickness and is often combined with macrocytosis;
- polychromatophils - red blood cells, colored in a blood smear in a light purple, lilac color. With a special supravital stain, these are reticulocytes. Normally, they can be single in a smear.
Anisochromia of erythrocytes is different colors of individual erythrocytes in a blood smear.
Blood chemistry
With the development of IDA, the following will be recorded in a biochemical blood test:
- decrease in serum ferritin concentration;
- decrease in serum iron concentration;
- increase in life expectancy;
- decrease in transferrin saturation with iron.
Differential diagnosis
When diagnosing IDA, it is necessary to carry out a differential diagnosis with other hypochromic anemias. Iron redistribution anemia is a fairly common pathology and in terms of frequency of development it ranks second among all anemias (after IDA). It develops in acute and chronic infectious and inflammatory diseases, sepsis, tuberculosis, rheumatoid arthritis, liver diseases, cancer, ischemic heart disease, etc. The mechanism of development of hypochromic anemia in these conditions is associated with the redistribution of iron in the body (it is located mainly in the depot) and a violation mechanism for recycling iron from the depot. In the above diseases, activation of the macrophage system occurs, when macrophages, under activation conditions, firmly retain iron, thereby disrupting the process of its reutilization. A general blood test shows a moderate decrease in hemoglobin (<80 g/l). The main differences from ZhDA are:
- increased level of serum ferritin, which indicates increased iron content in the depot;
- serum iron levels may remain within normal limits or be moderately reduced;
- The CVS remains within normal values or decreases, which indicates the absence of serum Fe starvation.
Iron-saturated anemia develops as a result of a violation of heme synthesis, which is caused by heredity or can be acquired. Heme is formed from protoporphyrin and iron in erythrokaryocytes. In iron-saturated anemia, the activity of enzymes involved in the synthesis of protoporphyrin occurs. The consequence of this is a violation of heme synthesis. Iron, which was not used for heme synthesis, is deposited in the form of ferritin in macrophages of the bone marrow, as well as in the form of hemosiderin in the skin, liver, pancreas, and myocardium, resulting in the development of secondary hemosiderosis. A general blood test will record anemia, erythropenia, and a decrease in color index. Indicators of iron metabolism in the body are characterized by an increase in the concentration of ferritin and serum iron levels, normal indicators of life-saving blood test, and an increase in transferrin saturation with iron (in some cases reaching 100%). Thus, the main biochemical indicators that allow us to assess the state of iron metabolism in the body are ferritin, serum iron, total body mass and % transferrin saturation with iron. Using indicators of iron metabolism in the body allows the clinician to:
- identify the presence and nature of iron metabolism disorders in the body;
- identify the presence of iron deficiency in the body at the preclinical stage;
- carry out differential diagnosis of hypochromic anemia;
- evaluate the effectiveness of the therapy.
Principles of classification of anemia
There are several types of classifications of anemia, based on a number of signs - the cause of the disease, the mechanism of its development, stages, symptoms and other parameters. The following groups are distinguished:
Sign up for an anemia screening
Make an appointment
Treatment
See also: Iron supplements
Treatment is carried out only with long-term intake of ferrous iron preparations orally in moderate doses, and a significant increase in hemoglobin, unlike improvement in well-being, will not be immediate - after 4-6 weeks.
Usually, any preparation of ferrous iron is prescribed - most often it is ferrous sulfate - its prolonged dosage form is better (sorbifer durules, tardiferon), in an average therapeutic dose for several months, then the dose is reduced to a minimum for several more months, and then (if the cause of anemia is not eliminated ), the maintenance minimum dose continues to be taken for a week, monthly, for many years. Thus, this practice has proven itself well in the treatment of women with chronic posthemorrhagic iron deficiency anemia due to long-term hyperpolymenorrhea with sorbifer and tardiferon - one tablet in the morning and evening for 6 months without a break, then one tablet a day for another 6 months, then for several years every day for a week. days of menstruation. This provides an iron load during the appearance of prolonged, heavy periods during menopause. A senseless anachronism is determining hemoglobin levels before and after menstruation.
For agastric (gastrectomy for a tumor) anemia, a good effect is achieved by taking a minimum dose of the drug continuously for many years and administering vitamin B12 200 micrograms per day intramuscularly or subcutaneously for four weeks in a row every year for life.
Pregnant women with iron deficiency and anemia (a slight decrease in hemoglobin levels and the number of red blood cells is physiological due to moderate hydremia and does not require treatment) are prescribed an average dose of ferrous sulfate orally before birth and during breastfeeding, unless the child develops diarrhea, which usually happens rarely.
Cost of consultation for anemia?
| Name of service | Price, rub.) |
| Initial appointment with a cardiologist | 1800 rub. |
| Repeated appointment with a cardiologist | 1300 rub. |
| Primary appointment with a general practitioner | 1800 rub. |
| Repeated appointment with a general practitioner | 1300 rub. |
| Prescription of treatment (drawing up an individual treatment regimen) | 1000 - 2500 rub. |
All our services and prices
Literature
- Vorobyov A.I. Guide to hematology. Moscow., “Medicine”. 1985.
- Dvoretsky L.I. Iron deficiency anemia. Moscow., "Newdiamed", 1998, p. 37.
- Conrad M. E. Iron Overloading Disorders and Iron Regulation. Seminars in Hematology. W. B. Saunders Company. 1998, v 35, n1, 1-4.
- Umbreit JN, Conrad ME, Moore EG and Latour LF Iron Absorption and Cellular Transport: The Mobilferrin \ Paraferritin Paradigm. Seminars in Hematology. WB Saunders. 1998, 35, 1, 13-26.
- Perkins Sherrie L. Normal blood and bone marrow values in humans. In Wintrobe's Clinical Hematology. eds Lee GR, Foerster J., Lukens J., Paraskevas F., Greer JP, Rodgers GM 10th ed. l998, v 2, p 2738-41, Williams & Wilkins.
- Wharton BA Iron Deficiency in Children: Detection and Prevention. Review. British Journal of Haematology 1999, 106, 270-280.
Iron in the human body
Iron deficiency anemia (IDA) is the most common form of all currently known anemias, which is due to a large number of reasons and circumstances that can lead to iron deficiency, which will lead to various disorders that are unsafe for the body.
Iron (ferrum, Fe) is a very important element for ensuring the normal functioning of the human body.
Men (of average height and weight) contain approximately 4 - 4.5 grams:
- 2.5 - 3.0 g is in heme Hb;
- in tissues and parenchymal organs, from 1.0 to 1.5 g (approx. 30%) is deposited as a reserve - ferritin;
- myoglobin and respiratory enzymes take up 0.3 - 0.5 g;
- some proportion is present in ferrum transport proteins (transferrin).
Daily losses in males, of course, also occur: every day about 1.0-1.2 g of iron leaves the intestines.
In women, the picture is somewhat different (and not only due to height and weight): their iron content is in the range of 2.6 - 3.2 g, only 0.3 g is deposited, and losses are not only daily through the intestines. Losing 2 ml of blood during menstruation, the female body loses 1 g of this important element, so it is clear why a condition such as iron deficiency anemia occurs more often in females.
In children, the levels of hemoglobin and the iron it contains change with age, however, in general, up to one year of age they are noticeably lower, and in children and adolescents under 14 years of age they approach the female norm.
The most common form of anemia is IDA due to the fact that our body is generally incapable of synthesizing this chemical element and, except from animal products, we have nowhere else to get it. It is absorbed in the duodenum and slightly along the small intestine. Ferrum does not interact with the colon in any way and does not react to it, therefore, once there, it passes through in transit and is excreted from the body. By the way, there is no need to worry that by consuming a lot of iron with food, we can “overeat” it - humans have special mechanisms that will promptly stop the absorption of excess iron.
Complications
The progression of the pathological condition and the lack of drug and dietary correction can cause the following complications:
- anemic coma, developing due to critically low oxygen delivery by red blood cells to brain cells;
- polyinsufficiency of internal organs, arising for the same reason;
- delayed intellectual and physical development, which can occur in children with severe iron deficiency;
- frequent viral diseases with the addition of bacterial flora and the risk of developing septic inflammation.
Hemolytic
This type of anemia is divided into types according to the following characteristics:
- hereditary disease (disturbances in the structure of blood cells, enzyme deficiencies, hemoglobinopathies);
- acquired forms (autoimmune, associated with mechanical damage to the bodies, toxic, etc.);
- destruction of red blood cells (hemolytic disease of newborns, idiopathic in lymphoma).
All types of hemolytic conditions require complex treatment under medical supervision, so you should not use folk remedies, aggravating the pathology.
Causes of the disease
Signs of pathology indicate iron deficiency. Such deficiency conditions develop with constant blood loss - 80% of all cases:
- bleeding from the gastrointestinal tract (ulcer, erosion, varicose veins of the esophageal veins, diverticulitis, hookworm, oncology, ulcerative colitis, hemorrhoids);
- heavy menstrual flow, erosion;
- long-term micro- and macrohematuria (pyelonephritis, urolithiasis, urinary oncology);
- bleeding from the nose, lungs;
- blood loss during hemodialysis;
- uncontrolled donation.
Other causes of the disease:
- Anemia due to impaired absorption (removal of part of the intestine, enteritis, problems with absorption).
- Increased needs (growth and development, pregnancy, lactation, physical activity, training).
- Deficiency disease with insufficient food intake (children, vegetarianism, strict diets, fasting).
To prevent IDA, it is recommended to consume at least 12 mg of the element daily.
Aplastic
With this disease, the growth and maturation of all types of blood cells (platelets, lymphocytes, erythrocytes and leukocytes) in the bone marrow is impaired. The development of pathology can be provoked by:
- exposure to salts of heavy metals, arsenic and benzene hydrocarbons;
- influence of radiation;
- taking medications (cytostatics, Levomycetin, Analgin, etc.);
- infections;
- autoimmune diseases (lupus erythematosus, etc.).
Like all types of anemia in adults, aplastic anemia is expressed by anemic syndrome. In addition, it is characterized by:
- increased bleeding;
- the appearance of hemorrhages;
- infectious complications;
- Blood tests reveal tricytopenia, a strong decrease in hemoglobin, and an increase in ESR.
The classification of anemia of this type is carried out in a clinical setting; treatment can only be prescribed by a doctor. Sometimes the spleen is removed or a bone marrow transplant is required.
Prevention
To prevent the development of iron deficiency anemia, experts advise:
- adhere to the principles of rational nutrition with the inclusion of a sufficient amount of meat products in the menu;
- preventive administration of iron supplements to patients at risk;
- Carrying out thorough correction of bleeding using medicinal or surgical methods.
Hemolytic anemia Aplastic anemia Endometriosis Pancreatitis Hypothyroidism Hepatitis C: first signs and treatment regimen