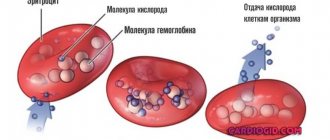
Multiple organ failure syndrome develops as a result of simultaneous or sequential dysfunction of several organs. In most cases, multiple organ failure is the terminal stage of serious diseases, including the last stages of cancer. The term was introduced relatively recently - in 1973 and for more than 45 years it continues to be one of the most common causes of death among patients in intensive care units.
- Features of multiple organ failure
- How does multiple organ failure syndrome manifest?
- Why does multiple organ failure develop?
- Methods for diagnosing the disease
- Treatment methods
- Why is multiple organ failure dangerous?
What it is
Multiple organ failure is a disease that is a complex pathological condition of a person, the peculiarity of the course is due to the dysfunction of 1 or 2 human organs (usually a child or teenager). In 80% of cases, the disease leads to high mortality , especially if timely treatment and diagnosis are neglected.
Multiple organ failure is characterized as the basis for the appearance of a critical indicator of the physiological processes of the body. The degree of damage directly depends on the ability of the human body to resist pathogenic factors and microorganisms.
Diagnostics
Diagnosis, in this case, is purely individual, since everything depends on the current condition of the patient. Urgent resuscitation is often required to stabilize the patient's condition.
Diagnostic methods depend on the current symptoms of organ failure. The following must be carried out:
- general and biochemical blood test;
- general urine analysis;
- coprogram;
- CT, MRI;
- Ultrasound of internal organs;
- HIV test.
Treatment will depend on the identified disorder, the underlying factor, and the patient's current condition. Quite often, if MODS is diagnosed in the second stage of development, only maintenance therapy is carried out.
Clinical picture
Clinical manifestations of multiple organ failure affect almost every system of the body. At the first signs of the development of multiple organ failure, activators of damage to functional systems affect the generalized system-wide response.
In this case, the following clinical characteristics appear:
- Fever, temperature from 37-38 degrees.
- The pulse increases to 90-95 beats per minute.
- The frequency of breaths increases more than 20 times per minute.
- Arterial hypocapnia – less than 32 mm Hg. Art.
- Leukopenia – less than 4000 mm.
- Leukocytosis – 12000 mm.
Multiple organ failure (what it is and how it manifests itself - knowledge that saves a person’s life) begins abruptly, the temperature rises suddenly. Depending on the strength of the body, chills, vomiting, and severe headaches may occur. The severity of symptoms is influenced by the fact which specific systems are affected by the disease.
After medical laboratory tests, the presence of multiple organ failure is indicated by the following characteristics:
- Dysfunction of hemostasis, with fibrinogen degradation more than 1/40, prothrombin index less than 70%, platelets less than 150 g/l.
- Acute respiratory syndrome, in which bilateral pulmonary infiltrates are observed.
- Renal dysfunction, in which blood creatine is more than 0.176 mmol/l, sodium in urine decreases to 40 mmol.
- Liver failure, in which AST and ALT increase 2 times higher than normal.
- Disorders of the central nervous system are diagnosed using the Glasgow scale - less than 15 points.
Comprehensive diagnostics makes it possible to identify changes in the patient’s condition, as well as his independent ability to resist disorders in the body.
Symptoms
With MODS syndrome, the following clinical picture is observed:
- breathing problems, shortness of breath;
- rapid or rare pulse;
- pallor, yellowing or blue discoloration of the skin;
- feeling of coolness in the lower and upper extremities;
- signs of oligo- or anuria (fluid retention in the body);
- yellow sclera and other visible mucous membranes;
- itching of the skin, which gradually increases;
- formation of subcutaneous hematomas and bruises;
- symptoms of acute heart failure;
- signs of dyspeptic disorders;
- lethargy.
It should be noted that it is not always possible to observe the full manifestation of the clinical picture of MODS. Depending on the etiological factor and the general condition of the patient, at any stage of development of complications, both coma and death can occur.
Impact of infection
Multiple organ failure: what is it, what are the causes - occurs against the background of primary infectious lesions. The primary foci of inflammation are the respiratory organs (bronchi, lungs) and peritonitis. If, with the development of multiple organ failure, a septic infection is added, which develops in the first 2-3 days, serious health complications may begin.
If an infection is added, the chances of recovery and life are significantly reduced, although with timely diagnosis and proper treatment, the patient can survive.
Causes of the disease in newborns
Multiple organ failure: what it is, what factors contribute to its development, it is important to understand before starting therapy. Most often it occurs in conjunction with pathological changes in the functions of organs and physiological systems. This can be observed after injuries, acute illnesses, shock, etc.
The list of reasons that can cause this condition includes:
- Ulcers and colitis.
- Serious life-threatening injuries.
- Severe skin wounds.
- Severe course of infectious processes.
- Large amount of blood loss.
- Severe food or alcohol poisoning.
- State of shock.
- Diabetic complications.
- Asystology.
- Eclampsia.
- Sepsis.
- Coma.
- HIV infection, AIDS.
- The period after chemotherapy.
- Blood mismatch (factor, group) after transfusion.
Factors in the development of such problems also include extreme stress and severe human conditions.
Multiple organ failure is included in a number of systemic diseases. There are a number of etiological factors that can become catalysts.
They are:
- Alcohol binges (perennial).
- Tobacco use.
- Long period of taking steroids.
- Use of cytostatic drugs in therapy.
- Wrong diet.
Often, a syndrome of complex pathology occurs when there is a sharp decrease in the body’s defenses after suffering severe infectious diseases.
Hypercatabolism in systemic inflammation syndrome, sepsis and multiple organ failure
According to the classic definition today by R. Bone (1997), the term sepsis is understood as “a systemic inflammatory response that occurs during an infectious process.” At the same time, the concept of “systemic inflammatory response syndrome” (SIRS) reflects an uncontrolled inflammatory response with generalized damage to tissue structures, caused by excessive production of pro-inflammatory mediators, primarily the tumor necrosis factor TNF-α, interleukins IL-1β, IL-6 and IL-8 . In 1998, M. Vervolet expressed the opinion that “... these mediators (including proinflammatory cytokines - M.E.) are largely, if not completely, responsible for the clinical manifestations and symptoms of a septic state in response to bacterial infection "(Fig. 2. 11.). Indeed, studies of the last decade of the last century have shown that in patients with sepsis the concentrations of circulating TNF-α, TNF receptor 1, IL-1β, and antagonists to IL-1, IL-6, and NFκB receptors were significantly increased. Moreover, high concentrations of pro-inflammatory cytokines clearly correlated with a high probability of death.
Experimental studies in animals have also confirmed the fact of an excessive increase in the level of pro-inflammatory cytokines in response to the introduction of bacterial endotoxins into the systemic circulation. Early studies by R. Beutler et al. (1985), H. Alexander et al. (1991) and A. Marchant et al. (1994) found an increase in the survival rate of experimental animals in a sepsis model when they were administered anti-cytokine immunoglobulins, cytokine receptor antagonists and anti-inflammatory cytokines (for example, IL-10). However, at the same time, studies by M. Eskandari et al. (1992), S. Opal et al. (1996) and C. Fisher et al. (1996) showed that not all septic patients had an increase in the concentration of TNF-α or IL-1β. Moreover, it was found that blocking TNF-α, both experimentally and in clinical studies, significantly worsened survival in sepsis.
It is known that the septic state itself is associated with more or less pronounced immunosuppression: the concentration of IL-10 and IL-4 increases, the production of interferon ϒ by T helper cells, the expression of HLA by monocytes, their proliferative and secretory activity of T lymphocytes decreases. A very common point of view is that sepsis begins with a phase of hyperinflammation, which is manifested by the development of SIRS. The inflammatory response is then limited by the compensatory anti-inflammatory system (CARS - Counter Anti-inflammatory Response System), which results in a state of immunosuppression. At the same time, there is a reasoned opinion that pro- and anti-inflammatory activity develop synchronously. In this regard, it is obvious that both uncontrolled hyperactivation of the production of proinflammatory cytokines and their complete inactivation equally determine critical disruption of homeostasis and death of the body. In the first case, excessive SIRS causes generalized endothelial damage, systemic hypoperfusion and multiple organ failure. In the second case, additional external stimulation of the compensatory anti-inflammatory system leads to immunosuppression and the natural development of exo- and endogenous infection. The SIRS – CARS balance is very unstable and depends on a number of factors: the prevalence and area of primary damage, the severity of contamination and pathogenicity of microflora, individual differences in the production of pro-inflammatory cytokines, the sensitivity of tissues to their damaging effects, as well as to the inhibition of their activity.
Multiple organ failure syndrome (MODS) is a natural completion of systemic disorders that developed in the process of SIRS. MODS is currently understood as a severe nonspecific stress reaction of the body, failure of two or more functional systems, universal damage to all organs and tissues of the body by aggressive mediators of a critical condition with a temporary predominance of symptoms of one or another organ failure - pulmonary, cardiac, renal, etc. The main feature of MODS is the uncontrollable development of damage to a life-support organ or system to such a depth, after reaching which it is necessary to state the inability of the organ to function in the interests of maintaining vital functions in general and preserving its structure in particular. The immediate factors that determine the severity of multiple organ dysfunction are the different ability of organs to withstand hypoxia and decreased blood flow, the nature of the shock factor and the initial functional state of the organ itself.
Etiologically, SIRS and MODS can be post-traumatic, post-hemorrhagic, septic, pancreatogenic or post-resuscitation. It is quite obvious that the presence of systemic inflammatory response syndrome in surgical patients is noted not only with the development of a septic condition. SIRS is an inevitable companion and an integral part of the pathogenesis of any extensive traumatic injury, including surgical trauma (see Fig. 2. 12.). However, in almost 90% of cases, MODS is of an infectious nature with a mortality rate ranging from 35 to 75% or more.
There are three main phases in the development of MODS:
- induction phase, the result of which is the synthesis of a number of humoral factors that trigger a systemic inflammatory response;
- cascade phase, accompanied by the development of acute pulmonary injury, activation of cascades of the kallikrein-kinin system, arachidonic acid system, blood coagulation system and others;
- the phase of secondary autoaggression, extremely pronounced organ dysfunction and stable hypermetabolism, during which the patient’s body loses the ability to independently regulate homeostasis.
The initiating factor that triggers the release of systemic inflammatory mediators can be of very different origins - infection, trauma, ischemia, blood loss, burns. The listed influences transfer polymorphonuclear cells (neutrophils, basophils, granulocytes) and endothelial cells into a state of “oxygen explosion”; the result of this transformation is a powerful chaotic release of a huge number of substances into the bloodstream by these cells that have multidirectional effects and are mediators of MODS (see Table 1) .
Table 1. Mediators of MODS.
Cytokines:
Eicosanoids:
Mediator amines:
Opioids/neurotransmitters:
| Hormonal amines/peptides:
Complement Kinins Fibronectin Growth factors Enzymes:
Nitric oxide (NO) Products of lipid peroxidation (LPO):
|
The main factors aggravating the “mediator-cytokine storm” are hypoxia and disoxia, deep microcirculation disorders, abnormally high concentrations of intermediate and final metabolic products, circulating immune complexes, biogenic amines, and peroxidation products. A number of studies have confirmed that the basis for the pathogenesis of MODS is a disseminated inflammatory reaction, accompanied by the activation and release of a large number of biologically active compounds. MODS should be considered the most severe degree of SIRS—generalized inflammation that causes damage to organ function.
In the light of modern ideas about the systemic inflammatory response, there are two main pathways for the development of MODS. Primary MODS (early multiple organ failure) is a direct result of exposure to a certain damaging factor of any etiology. At the same time, signs of organ dysfunction appear early. An example of this type of MODS can be multiple organ dysfunction in polytrauma or severe burns.
Secondary MODS (late multiple organ failure) develops after a latent phase and is the result of a generalized systemic response of the body to a damaging factor. The septic variant of MODS can be considered as a classic secondary organ failure, a manifestation of an extremely severe systemic response to infectious invasion.
The studies carried out made it possible to identify the general pattern of the formation of MODS. In most cases, in the most general form, the sequence of system involvement in MODS is as follows:
- respiratory distress syndrome;
- encephalopathy;
- renal dysfunction syndrome;
- liver dysfunction syndrome;
- stress ulcers of the gastrointestinal tract.
Metabolic stress, caused by activation of the sympatho-adrenal system and the release of a colossal number of biologically active substances (biogenic amines, eicosanoids, interleukins, free radicals), determines the disruption of all types of metabolism with excessive mobilization of energy substrates in the processes of glycogenolysis, lipolysis, proteolysis and gluconeogenesis, which has its consequence is the development of insulin-resistant hyperglycemia and negative nitrogen balance.
The main feature of the entire set of metabolic changes described is the combination of the body’s hyper-need for various substrates to adapt to increased energy costs with tissue tolerance to the same substrates.
The most important role in the development of systemic metabolic disorders is played primarily by cytokines. The most pronounced metabolic effects are those of interleukin-6 and tumor necrosis factor, previously called “cachectin” (causing wasting). The effect of TNF-a on organs and tissues during the development of SIRS is shown in Table 2.
Table 2. Effects of tumor necrosis factor on tissues and cells (according to Vincent J. L, 1994)
| Textile | Effects |
| Endothelium |
|
| Muscle |
active breakdown of proteins |
| Liver |
|
| Brain |
|
| Connective tissue |
|
Most authors combine the described characteristics into a single syndrome of hypermetabolism (hypercatabolism, “autocannibalism”). It is the hypermetabolism syndrome that plays a leading role in the pathogenesis of multiple organ failure. The modern three-phase model of the pathogenesis of MODS considers hypermetabolism syndrome, on the one hand, as the main component of the formation of multiple organ dysfunction. On the other hand, it is the course of hypermetabolism syndrome, its correction or progression that determines the outcome in MODS.
At its core, hypermetabolism syndrome in SIRS, sepsis and MODS is an integrative metabolic response of the body to a generalized inflammatory response. Hypermetabolic multiple organ failure can occur under the influence of any etiological factor - acute blood loss, sepsis, polytrauma, ischemia, severe inflammatory-necrotic process (a typical example is severe acute pancreatitis, widespread peritonitis). All of the listed trigger elements lead to the development of systemic hypoperfusion with clinical symptoms of microcirculation disorders, hypotension, and oliguria.
Manifestations of hypermetabolism include a large number of clinical and laboratory indicators: fever, leukocytosis, tachycardia, tachypnea, increased cardiac output and, accordingly, cardiac index, decreased total vascular resistance, hyperglycemia, hyperlactatemia, increased oxygen consumption, urinary excretion of nitrogen more than 15 g per day. In addition, there is an increase in serum creatinine and bilirubin levels, and prerenal azotemia develops.
The main changes in the metabolism of proteins, fats and carbohydrates in SIRS can be presented as follows.
Protein metabolism:
- redistribution of proteins for gluconeogenesis, synthesis of acute-phase proteins, cytokines;
- despite increased protein synthesis, the breakdown of protein substances with a negative nitrogen balance predominates.
Carbohydrate metabolism:
- the tolerance of peripheral tissue cells to insulin and glucose is increased;
- the rate of glucose production by hepatocytes increases from 2.5 to 4.4-5.1 mg/kg/min;
- mobilization of amino acids from myocytes of skeletal muscles and visceral cells for gluconeogenesis;
- a combination of peripheral tissue tolerance to glucose and active gluconeogenesis.
Lipid metabolism:
- activation of lipolysis;
- decreased utilization of fatty acids and triglycerides by tissues;
- decreased lipoprotein lipase activity.
A global physiological characteristic of hypermetabolism is an increase in metabolic rate two or more times compared to the basal metabolism, which is accompanied by a significant increase in oxygen consumption, negative nitrogen balance, and hyperproduction of CO2.
It is obvious that the consequence of the progressive course of hypermetabolism is the occurrence of not only organ and multiple organ dysfunction, but also protein-energy deficiency with subsequent exhaustion (cachexia). Nevertheless, it should be understood that hypermetabolism and simple starvation - processes leading to nutritional deficiency - have fundamentally different functional and biochemical characteristics (see Table 3).
Table 3. Main characteristics of hypermetabolism and simple fasting
| Characteristics | Simple fasting | Hypermetabolism |
| Cardiac output | — | ++ |
| OPSS | without changes | —- |
| Consumption 02 | — | ++ |
| Energy requirement | — | +++ |
| Mediator activity | without changes | ++ |
| Response to regulatory stimuli | ++++ | + |
| Respiratory coefficient | 0, 75 | 0, 85 |
| Primary substrate | lipids | Lipids + carbohydrates + proteins |
| Proteolysis | + | +++ |
| Protein oxidation | + | +++ |
| Synthesis of acute phase proteins in the liver | + | +++ |
| Urogenesis | + | +++ |
| Glycogenolysis | + | +++ |
| Gluconeogenesis | + | +++ |
| Lipolysis | ++ | +++ |
| Ketonemia | ++++ | + |
| Rate of development of nutritional deficiency | + | ++++ |
| — reduction | + increase |
Simple fasting is a clinical situation in which the body receives nutrients (primarily proteins and calories) in quantities that are inadequate to the existing needs. The metabolic response to simple fasting is a specific adaptive reaction, the purpose of which is to reduce body weight loss, which is characterized by a decrease in resting energy requirements, utilization of alternative energy sources, and a decrease in protein breakdown. The main sources of nutrients during fasting are glycogen, fatty acids, ketone bodies, and glycerol. Protein metabolism is characterized by a decrease in protein synthesis and breakdown, which slows down the processes of gluconeogenesis. The respiratory coefficient during simple fasting ranges from 0.6-0.7, which reflects the body's use of lipids as the main sources of energy.
Unlike fasting, hypermetabolism is a generalized response that mobilizes energy and substrates to support inflammation, immune responses, and tissue regeneration. The increase in oxygen consumption and carbon dioxide production is a consequence of almost doubling the resting energy requirement. In contrast to simple fasting, the respiratory coefficient is 0.80-0.85, which is typical for the oxidation of various energy substrates. While there is a net increase in nutrient intake, including glucose, there is an absolute decrease in calories. obtained from the oxidation of glucose, and an increase in the amount of calories released from the oxidation of amino acids. A decrease in pyruvate intake causes a stoicheometric increase in the release of alanine and lactate, together with the oxidation of carbohydrate moieties of fatty acids and amino acids in the Krebs cycle. These characteristics reflect the activation of anaerobic glycolysis processes as an alternative way for the body to obtain energy.
The process of anaerobic glycolysis has specific differences from metabolism in a normally functioning organism: the presence of hyperalaninemia and hyperglutaminemia during the first three to four days of the disease due to the utilization of skeletal muscle amino acids for active gluconeogenesis; hyperlactatemia, hyperpyruvatemia and an increase in the lactate/pyruvate ratio due to suppression of pyruvate dehydrogenase activity and preservation of the normal redox potential of the cellular cytosol; hyperglycemia in non-diabetics, caused by the phenomenon of peripheral tissue tolerance to glucose. All these signs indicate a hypermetabolic restructuring of aerobic glycolysis processes.
The metabolism of carbohydrates, lipids and proteins has fundamental differences from metabolism under normal conditions and simple fasting. There is an increase in the activity of the processes of glycogenolysis and gluconeogenesis, and the introduction of exogenous glucose and insulin does not in any way affect the rate of biochemical reactions. The main substrates for gluconeogenesis are lactate, glutamine, alanine, glycine, serine and glycerol. Despite the increased production of glucose by hepatocytes, insulin synthesis does not increase, which leads to spontaneous hyperglycemia. At the same time, peripheral tissues continue to release large amounts of lactate into the systemic circulation for glucose synthesis in the liver. Lactate also serves as the main energy fuel for myocardiocytes. Excessive intake of glucose into the body (more than 5 g/kg/day) leads to hyperosmolar syndrome, fatty infiltration of the liver, and increased carbon dioxide production.
Glucose homeostasis is regulated by several physiological control mechanisms to balance glucose uptake and production. However, hyperglycemia is a characteristic feature of the septic condition. Proinflammatory cytokines potentiate the release of other cytokines, mediators and catabolic hormones. These catabolic hormones—glucagon, catecholamines, and cortisol—stimulate glycogenolysis and glucose mobilization. Glucagon-stimulated glycogenolysis solves the problem of glucose mobilization only for a while. Glycogen stores are quickly depleted, and endogenous lipids, especially triglycerides, become the main source of energy. Circulating insulin levels may be normal or even low, but in most cases they are elevated. Maximum insulin efficiency is reduced by approximately 50% of normal (the phenomenon of insulin resistance). Gluconeogenesis increases with the progression of organ failure, as does the rate of lactate and pyruvate formation. On the other hand, hypoglycemia and decreased glucose synthesis can also be observed in severe sepsis, since these patients always have impaired liver function and/or decreased visceral blood flow.
Lipid metabolism in SIRS, sepsis and MODS is characterized by increased lipolysis and inhibition of lipogenesis. The turnover of long and medium chain fatty acids increases. The plasma profile of fatty acids changes: the concentration of olic acid increases, and linolenic and arachidonic acid decreases. The clearance of long-chain triglycerides is reduced by inhibition of lipoprotein lipase activity in adipose tissue and skeletal muscle.
Catabolic hormones are the main stimulators of triglyceride hydrolysis (lipolysis) by activating hormone-sensitive lipase. The so-called sepsis-induced lipolysis occurs as a result of the direct effect of catecholamines, which increase the activity of hormone-sensitive lipase. This can be explained by the suppression due to intense a2-vasoconstriction of the release of fatty acids from lipid stores. In the early phase of sepsis and starvation, catabolic hormones override the action of anabolic hormones (insulin), which leads to the breakdown of lipids into triglycerol and free fatty acids (FFA). The intracellular transport of long-chain FFAs across the mitochondrial membrane with the participation of carnitine is disrupted. Due to the accumulation of long-chain FFA esters, inhibition of the function of the pyruvate dehydrogenase complex directly occurs, which leads to intracellular acidosis and the accumulation of lactate and pyruvate. The clearance of long-chain triglycerides (TGs) is reduced by inhibition of lipoprotein lipase activity in adipose tissue and skeletal muscle. Adipose tissue breaks down into fatty acids, which enter the systemic circulation and then into the liver. Inadequate tissue perfusion can inhibit the lipolysis process. The release of cytokines helps to reduce the utilization of fatty acids and TG by suppressing the activity of lipoprotein lipase.
The septic condition leads to an increase in the concentrations of free fatty acids in the early stages of the catabolic reaction. However, this phenomenon does not always occur with different etiologies of catabolism. High concentrations of free fatty acids are the result of the release of these substances from depots in adipose tissue, which confirms the fact that the rate of lipolysis predominates over re-esterification processes. The rate of uptake of free fatty acids by peripheral tissues is directly proportional to the plasma concentration of these substances. Increased mobilization of lipid molecules is used by the body against the background of a catabolic reaction to meet the metabolic needs of both cardiac and skeletal muscles, as well as to reduce tissue consumption of monosaccharides. The energy obtained from lipid oxidation is spent primarily on the intrahepatic synthesis of glucose from triatomic precursors such as lactate (produced from the breakdown of muscle glycogen and glycolysis) and alanine (a product of muscle proteolysis).
In addition to a decrease in FFA utilization in sepsis, ketogenesis worsens with the occurrence of a deficiency of ketone bodies, which are an important source of energy for peripheral cells. Finally, the activity of lipoprotein lipase decreases, which, together with other factors, determines the increase in hyperlipidemia, hyperglycemia, and hyperlactatemia.
During the systemic inflammatory response, protein catabolism increases significantly. Despite the accelerated synthesis of proteins, the reactions of protein breakdown and consumption create a negative nitrogen balance and contribute to a progressive decrease in body weight (autocannibalism). Amino acids are mobilized from skeletal muscle, connective tissue, and non-functioning intestines and support the wound process, cellular inflammatory reactions and the synthesis of “acute-phase” proteins. The absorption of amino acids by the liver and the synthesis of protein in it are increased. However, the rate of synthesis of different proteins in the liver increases unevenly. The synthesis of acute-phase proteins is increased, but the synthesis of those proteins that are synthesized almost exclusively in the liver (for example, albumin and transferrin) is decreased. The rate of urea formation is increased, as is the rate of synthesis of creatinine, uric acid and ammonia, all of these substances are excreted in the urine in increased quantities. The daily excretion of amino acids in urine reaches 25-30 g and is not fully corrected by parenteral administration of nitrogen and energy donors.
Additionally, there are processes of redistribution of amino acids and an increase in the rate of their oxidation, especially in skeletal muscles. Unlike catabolic processes, the rate of protein synthesis is reactive to the input of exogenous amino acids and energy. In this case, the required amount of amino acids is 1.5-2 g/kg/day. Some of the mobilized amino acids become a substrate for oxidation. Moreover, even under the conditions of the introduction of exogenous glucose, the mobilization of amino acids continues. One of the reasons for this process is the need to provide enterocytes and leukocytes with glutamine, which they need as a substrate for oxidation. Continued proteolysis in skeletal muscles worsens respiratory function, in the integumentary tissues it prolongs the first phase of the wound process, aggravates immunosuppression, accelerates the loss of muscle strength, significantly delays the recovery period and ultimately increases the risk of death of the patient.
Biochemical reactions in the process of hypermetabolism create many vicious circles, the interaction of which results in loss of structure and pronounced energy imbalance in the cell. This is confirmed by morphological studies of skeletal muscles in patients with SIRS, in whose biopsies a decrease in ATP content and an increase in adenosine diphosphate and adenosine monophosphate were established.
Thus, SIRS, sepsis and MODS are characterized by increased energy expenditure, hypercatabolism in both internal organs and skeletal muscles, and increased demand for fat depots. At the beginning, such a hypermetabolic reaction may even be beneficial, since it is a component of the systemic adaptive response and a protective anti-infective factor. However, the prolonged existence of a hypermetabolic state becomes dangerous. Nutritional support alone cannot change the rate of catabolism, but it can accelerate the rate of polymer synthesis, which gives patients an additional chance of stabilizing nutritional status and survival. However, to date, mortality rates for hypermetabolism syndrome remain unacceptably high, ranging from 25 to 40%.
© Evseev M. A., 2016
Development of the disease in the elderly
Among older people, the number of patients with multiple organ failure is several times higher. Often this condition occurs in conjunction with concomitant disorders and diseases. This seriously threatens human life and requires long-term maintenance of strength and vital functions.
Reasons for the development of multiple organ failure in older people:
- Injuries.
- State of shock.
- Coma.
- Septic infections.
Multiple organ failure (what it is, how to treat it in old age is determined by the doctor) is characterized by long hospitalization and a high mortality rate.
Methods for diagnosing the disease
Symptoms of multiple organ failure may be similar to other diseases, so to confirm the diagnosis, the doctor prescribes a comprehensive examination, which includes the following diagnostic methods:
- Examination of the patient, analysis of complaints, collection of anamnesis. Already at this stage, a specialist can notice characteristic signs that indicate damage to one or more organs. These may be disturbances in respiratory and cardiac activity, metabolic changes, and deviations in hemodynamics.
- Instrumental examination. Its volume depends on the manifestations of multiple organ failure. The doctor has all non-invasive methods at his disposal, for example, ultrasound, X-ray, CT, MRI, etc. In addition, it is important to regularly monitor the body’s vital signs - blood pressure, heart rate, respiratory rate, etc.
- Laboratory diagnostic methods. Usually, basic tests are prescribed that allow one to evaluate and further monitor the main indicators of hemodynamics, the level of electrolytes and enzymes in the blood, etc.
Taking into account the fact that patients in most cases are in an intensive care unit, multiple organ failure can be detected in the early stages, when complete failure of the organ or system has not occurred.
Symptoms of the disease
Factors that indicate the development of multiple organ failure may vary based on the stages of disease development, the type and combination of systems. In addition, the symptoms are influenced by concomitant diseases, infections and other factors.
Primary signs of the development of multiple organ failure syndrome:
- General loss of strength, malaise.
- Breathing problems.
- Increased heart rate.
- Coldness and numbness of the limbs.
- Dyspnea.
- Pale skin.
- The sclera becomes yellow.
Multiple organ failure may be characterized by yellow sclera. - Indigestion.
- Bruising.
Most symptoms of multiple organ dysfunction syndrome are similar to other diseases, so they are easy to miss. For an accurate picture and timely treatment, additional diagnostics in the laboratory are required.
For example:
- Pathological disorders of the respiratory system are accompanied by difficulty breathing and shortness of breath.
- Renal dysfunction leads to changes in characteristics in urine analysis.
- If multiple organ failure affects the liver, changes in bilirubin levels will be clearly visible in a blood test, and jaundice will also develop.
- When multiple organ failure affects the hemostatic system, thrombocytopenia and similar abnormalities will be observed.
- If the heart is affected due to this disease, hypotension develops, ventricular arrhythmia, and acute heart failure appear.
- Disorders of the gastrointestinal tract are characterized by the appearance of several foci of inflammation and perforation in the mucous membrane of the digestive tract.
- Damages to the organs of the central nervous system are characterized by the presence of acute psychosis and overexcitation.
Multiple organ failure is a disease that occurs in conjunction with the development of hemostatic dysfunction, which is caused by a deficiency of blood clotting and hyperstimulation.
DIC syndrome stimulates thrombotic disorders, hemorrhagic dysfunction, and inhibition of blood microcirculation. Basically, with DIC syndrome, dysfunction of some organs develops: subcutaneous hematomas, petechial-hematomal rashes on the body. In case of complications, shock, hypotension, and severe bleeding may occur.
One of the common manifestations of this systemic disease is acute heart failure. This is due to the fact that the elasticity and contractile properties of the cardiac sac muscle sharply decrease. As a result, the blood circulation process slows down and blood stagnation appears.
Without timely treatment, this syndrome can lead to swelling of the respiratory system and asthmatic attacks. These are extremely serious conditions that are life-threatening for the patient.
Forecast
Multiple organ failure syndrome is characterized by high mortality rates - from 27 to 100%, depending on which organs are affected and their number:
- with failure of one organ, up to 20% of patients die;
- with failure of two organs - up to 25%;
- with failure of three organs - 50%;
- with failure of four organs - 70–90%.
Hospital treatment continues for a long time, but even if it is completed successfully, complications often persist, such as coronary heart disease, pulmonary dysfunction, chronic renal failure, nervous system disorders, and heart rhythm disturbances due to blockades.
A patient discharged after treatment for MODS must subsequently be observed by a doctor, follow all his recommendations, receive treatment for complications, concomitant diseases, and generally be careful and attentive to his health.
Leading doctors at the Medicine 24/7 clinic use all available modern, innovative techniques for the treatment of multiple organ failure. Each patient in the intensive care ward is constantly monitored, and our resuscitators do everything necessary to maximize the chances of a successful outcome. Our clinic operates around the clock, we are ready to receive patients and provide emergency assistance at any time.
The material was prepared by Tatyana Evgenievna Dobrosotskaya, Deputy Chief Physician for ICU at the Medicine 24/7 Clinic.
Phases of development
Multiple organ failure (what it is and preventive measures is important to know before the disease develops) is divided into several main stages of its course.
They are:
- Induction – manifests itself as the synthesis of biologically active substances in the body, due to the stimulation of mediators that cause the launch of a response inflammatory process.
- Cascade - occurs in the form of uncontrolled acute lung injury syndrome, as well as activation of the kinin-kallikrein system, arachidonic acid. In addition, the level of fibrinolysis and accompanying hemostasis systems is significantly reduced.
- Secondary autogression and complete loss of homeostasis of the body. A rather complex course of the phase, characterized by long-term treatment and a high mortality rate.
Multiple organ failure - what is it, causes in adults, newborns, the elderly
Multiple organ failure
or
multiple organ dysfunction syndrome
(
MODS
) is a clinical manifestation of an uncontrolled severe systemic inflammatory response triggered by trigger factors such as an infectious or inflammatory process or injury. It is characterized by changes in the body's defenses and dysregulation of the inflammatory response and reactions of the human immune system.
Selecting a given state
into a separate nosological form became possible thanks to the progress of medical science and the widespread development of intensive care units. It was identified as a separate syndrome in the early 1970s, when advances achieved in the treatment of critical conditions made it possible to shed light on this fairly common and often fatal combination of sequentially developing pulmonary, hepatic and renal failure.
Progressive dysfunction of various organs
with subsequent deficiency complicates the course of a wide variety of diseases and, despite the progress that has been made in understanding the mechanisms underlying this condition, the mortality rate still remains very, very high.
Multiple organ dysfunction syndrome
(
SPOD
) is today the most common cause of prolonged treatment for surgical patients in intensive care units (more than five days) and the most common cause of death (in these patients).
It should be said that SPOD
must be distinguished from postoperative or post-traumatic isolated organ dysfunction, which has a different pathogenesis and is significantly different from SPOD in terms of prognosis for the patient's life.
a) Epidemiology of multiple organ failure
. Definitions of organ failure are based on two different types of criteria, namely quantitative changes in indicators of the function of certain organs and systems (for example, hypotension, acidosis, serum creatinine concentration) or treatments necessary to compensate for certain functions (for example , dialysis, ventilation, etc.).
Degrees of dysfunction of various organs
, ranging from subclinical changes in their physiology to obvious failure, coupled with the difficulty of monitoring the function of absolutely all affected organs, has led to the fact that there is still no consensus on the definition of organ failure and its corresponding clinical varieties. All this greatly complicates the conduct of epidemiological studies and assessment of treatment outcomes.
Lack of clear data regarding the incidence of PODS
Due to the lack of universal diagnostic criteria, many studies published to date have used different clinical or operational definitions of organ failure.
Analysis of published
To date, research suggests that SPOD, depending on the diagnostic criteria used and the age-sex composition of patients in intensive care units, occurs in 5-15% of patients requiring treatment in these units. The data on disease outcomes obtained in these studies are generally consistent with each other, with the mortality rate depending on the number of organs affected.
AIDS Clinic
can proceed according to two scenarios that differ from each other in such characteristics as the onset of the disease in relation to the main event triggering the pathological process, the duration of the disease and the sequence of development of organ disorders. The first scenario usually occurs when the respiratory system is directly affected by trauma or aspiration. In this case, the duration of the pathological process can be quite short and SPOD will develop here as a terminal condition preceding the death of the patient.
The second scenario is a more classic form
pathological process that develops, for example, in severe sepsis and begins with lung damage in the form of acute respiratory distress syndrome (ARDS). In this case, SPOD occurs already in the early stages of the disease, but the full clinical picture develops after about 7-10 days, when the course of the underlying disease is complicated by the addition of liver and then kidney failure.
Classification according to the form of the pathogenetic mechanism
Based on the mechanism of pathogenesis, the course of multiple organ failure syndrome may differ:
- For the 1st single-phase form, the course of the syndrome is characterized by the development of acute pathologies. So, for 1-2 days there is a disturbance in the metabolism of active substances, after which renal and liver failure is added. Dysfunction of the central nervous system, disruption of the cardiovascular system, hemostasis. In this case, pathological processes precede death or serious injury.
- The second stage of this syndrome, against the background of the pathogenesis mechanism, causes the development of a two-phase course of pathological processes. After the first stage, the patient may feel a sharp improvement in his condition, a temporary stabilization of well-being. This is observed until it adds to the symptoms of sepsis and infection. Subsequently, a septic infection develops for several days; if measures are taken in time, the patient can recover.
How does multiple organ failure syndrome manifest?
The exact set of symptoms depends on the damage to certain organs. As a rule, the most distinct signs are signs of dysfunction of the respiratory system. This may be evidenced by the following clinical manifestations:
- Dyspnea.
- Activation of accessory muscles during breathing.
- Cyanosis of the skin.
- Severe sweating.
- Impaired consciousness and lethargy in the later stages.
When the cardiovascular system is damaged, chest pain, various hemodynamic disorders, swelling of soft tissues and internal organs are noted. At the initial stage, there is pronounced tachycardia, up to 180 beats per minute. It develops to compensate for disturbances and is eventually replaced by bradycardia, in which the heart rate can drop to 40 beats per minute or even lower. In the later stages, the patient responds poorly to drugs that help normalize the activity of the cardiovascular system. This is one of the reasons why treatment of multiple organ dysfunction becomes difficult.
Disruption of the gastrointestinal tract in multiple organ failure is manifested by symptoms of mechanical compression of the intestine. These symptoms include:
- Violation of the process of defecation.
- Gas retention.
- Bloating and asymmetry of the abdomen.
- Vomit.
- Loss of appetite.
In some cases, gastrointestinal bleeding develops, which aggravates the course of the underlying disease and often causes the death of the patient.
Quite often the clinical picture contains signs that are characteristic of renal failure. First of all, this is a pronounced decrease in urine volume with the subsequent development of anuria, which is an indication for hemodialysis. In addition, patients exhibit a decrease in potassium levels in the blood, renal edema, water and electrolyte imbalance, etc.
What is the danger of multiple organ failure
In medicine, the syndrome is the body’s response to the course of complex, acute pathologies. Despite the primary etiology, the syndrome is accompanied by a failure of all important life support systems and human functioning. Complications of multiple organ failure can be phenomena that accompany pulmonary failure and severe kidney disease.
They are as follows:
- Dysfunction of the circulatory system.
- Development of hypoxia.
- Anemia.
- Weakness, fainting.
- Dysfunction of the process of formation of proteins and immunoglobulins.
- Uncontrolled forms of hyperglycemia.
- Heart failure.
- Thrombocytopenia.
- Elimination of the protective barrier of the walls of the digestive organs.
Despite the complexity of the course, multiple organ failure is a curable disease. By undertaking active and timely treatment, together with resuscitation measures, you can maintain health and save lives.
Pathogenesis
Speaking about the clinical picture, multiple organ failure syndrome should be divided into several key conditions:
- acute liver failure;
- dysfunction of the central nervous system;
- acute renal failure;
- adult respiratory distress syndrome;
- DIC syndrome (also called disseminated intravascular coagulation syndrome).
The complications listed above are the leading causes of death in intensive care units. Depending on how many organs are in a state of failure, the likelihood of death of patients changes.
Metabolic disorders can be identified as a key link that triggers the processes that result in acute multiple organ failure. This pathology is a response to systemic damage, regardless of what the initial etiological factor was (polytrauma, burns, infections, ischemia).
Multiple organ failure can also be identified as the final stage of the body's hypermetabolic systemic response to a specific injury, which is manifested by an acute pulmonary disorder leading to the development of liver and kidney failure, as well as dysfunction of other human organs.
In the terminal stage of the disease, pronounced catabolism can be observed. The reason for its occurrence is the serious condition of the patient with an irreparable energy deficiency. As a result, protein-dependent energy metabolism develops, which is based on the breakdown of proteins and activation of proteolysis of muscle tissue, as well as vital organs. The consequence of this process is the release of substances by activated microbial and viral toxins, macrophages and mast cells that provoke cellular and tissue damage.
In this case, as a result of trauma, patients may develop a systemic inflammatory response syndrome, the severity of which depends on the volume of the affected tissue, the degree of shock and the innate properties of the body itself.
Disease prognosis
The degree and complexity of the syndrome is determined using the MOF (Multiple Organ Failure) scale specially developed for this purpose.
In this case, 7 life support systems of the body are assessed:
- Respiratory.
- Urinary.
- Hematological.
- Central nervous system.
- Digestive (gastrointestinal organs).
- Liver organs.
- Cardiovascular.
The forecast for the future and recovery are based on the number and degree of damaged organs and body systems.
So statistics provide the following data:
- 1 organ system – 20% mortality.
- 2 organ systems – 25-30% mortality among older people.
- 3 systems – more than 50% of deaths.
- 4 or more systems – 70-80% of patient mortality.
There are also possible consequences of multiple organ failure, such as:
- With secondary infectious lesions there is a high risk of mortality (especially in children).
- Complete or partial failure of the functioning of internal organs.
- Leveling of medical procedures, for example, hemodialysis.
Treatment methods
The main goal of patient treatment is to restore lost functions, eliminate the negative consequences of multiple organ failure and prevent complications. For this purpose, medications from the group of antibiotics, NSAIDs, hormones, anticoagulants, etc. are prescribed. If necessary, transfusions of blood or its components are performed, and prevention of disseminated intravascular coagulation syndrome, internal bleeding, and collapse is carried out. Throughout the treatment, the patient must observe strict bed rest.
In severe cases, surgical treatment methods are used. These include extracorporeal detoxification, elimination of intestinal obstruction, and removal of non-viable organs that have begun to become necrotic.
Treatment method
Before prescribing treatment, it is necessary to conduct laboratory tests and studies that will show the extent and area of the syndrome. For this purpose, only laboratory tests are used.
Multiple organ failure: diagnosis and, directly, what it is is confirmed by the formation of several signs of progression of the pathology of the functions of systems and organs. For example, damage to hemostasis and severe respiratory failure, or, for example, renal and liver failure.
Treatment of the syndrome occurs in a comprehensive manner, including several main areas:
- Prevention of the syndrome occurs through timely diagnosis and determination of the limit of development of the pathology. This is the main prevention of this syndrome; for this it is necessary to carry out a functional assessment of the body’s performance, monitoring and eliminating the development of infections. In the hospital, the circulatory system is normalized until hemostasis pathologists cross a critical point. It is also very important to carry out restoration measures of the respiratory system, treatment of necrosis, severe injuries and damage.
- The second principle of quality treatment is phasing and precise sequence of actions. The most effective treatment regimen includes artificial medicinal and therapeutic maintenance of the functioning of the affected system. Replacement of failed organs is effective. Often this applies to the respiratory and circulatory organs, enhancing the performance of physiological mechanisms, treating affected organs and areas. Therapy to eliminate the patient's state of shock.
- Antimediator property, which consists of therapy aimed at stopping the performance of endothelial cell receptors and antagonists of their work. For this purpose, monoclonal antibodies against TNFa IL-1 are mainly used.
- Restoring normal levels of energy balance. For this, a whole scheme of measures is used: changes in the metabolic process, creation of an acid-base balance, normalization of the performance of the enzyme system. They also prescribe nutrition to the body using a special probe, the introduction of vitamins, amino acids, and artificial enrichment of tissues with oxygen. The course of therapy includes restoration of normal functioning of the pulmonary and circulatory system, drug antihypoxic and antioxidant treatment of the patient.
- Therapy for eliminating toxins and their harmful effects, namely stimulating natural detoxification. For this purpose, intra- and extracorporeal methods are used in hospital settings.
- Syndrome therapy. For this, the components of the acute multiple organ failure syndrome, for example, hypovolemia, clotting problems, distress syndrome, acute liver disease, require an individual approach for all patients. Therapies are designed to eliminate symptoms, including drug replacement and support of certain vital organs.
- Reduced invasiveness. A comprehensive technique that includes the invasiveness of innovative technologies to reduce the severity of symptoms. Otherwise, complications associated with this syndrome can lead to iatrogenic multiple organ failure. Despite this, many doctors refuse invasive methods, because in addition to their benefits, they conceal a real threat to the life and health of the patient.
At the second stage of recovery, the following treatment may be prescribed:
- Artificial ventilation (if there are breathing problems).
- Use of cardiotonic drugs.
- Purification of blood from toxins, heavy metals (droppers).
- Hemodialysis.
- Maintaining heart rate using artificial methods.
The duration of complex treatment measures directly depends on the degree of complexity and the number of affected organs, lasting from 7 to 20 days. The age of the patients is of no small importance.
Preventive measures play an important role, especially in the management of severe patients who have a high likelihood of developing this syndrome.
Preventive techniques are the ideal choice of therapeutic intervention for victims in complex critical conditions. Particularly difficult pathologies occur against the background of this syndrome, such as acute forms of infectious inflammation and blood loss.
The complex of preventive measures provides for systematic diagnosis, examination, and treatment of pathological, chronic processes in the body. In addition, it is important to ensure support for all functions of the body as a whole, to enrich tissues with microelements and vitamins in order to prevent irreversible effects and further long-term treatment.
The effectiveness of the chosen method directly depends on the correct assessment of the condition and timely diagnosis of the number of affected systems and organs.
When treatment is preventive, precautionary in nature, the risk of death is significantly reduced and the patient’s recovery is possible. Awareness of the mechanisms of pathophysical processes allows us to timely determine the development of multiple organ failure syndrome and undertake well-constructed treatment tactics.
Multiple organ failure: how it manifests itself, what it is, what are the causes of development - the most important information for those who are predisposed to the disease. It is a group of systemic diseases in which there are dysfunctions of 2 or more organs.
This condition occurs equally in both adults and children. The peculiarity of the development of multiple organ failure is that the organs and systems of the human body are damaged so much that they can completely fail, are unable to perform functions and tasks, and support human life.
Article design: Oleg Lozinsky
Causes
Multiple organ failure can result from tissue hypoperfusion or hypermetabolism, various injuries and infections. As for cellular changes, the influence of mediators plays a major role in them. Their quantity during release depends on the severity of the factor provoking the damaging effect.
In some cases, the cause of multiple organ failure is a transfusion of canned blood that has been stored for a long time (especially in large quantities). Sometimes this condition is preceded by unskilled artificial ventilation. In the field of surgery, infectious complications are a key cause of the body's stress response. They cause disruption of the patient's homeostasis and metabolism system. In 7–22% of cases, multiple organ failure occurs in the postoperative period. In 50% of cases, the diagnosis is made due to purulent complications of acute inflammatory pathologies.
Multiple organ failure can result from impaired immunity and septic processes. In most situations, sepsis begins due to exposure to gram-negative bacteria that enter the organs and bloodstream through the gastrointestinal tract.