The time has come for summer holidays, which is also the long-awaited season of fresh berries, vegetables and fruits, swimming in the gentle waters of rivers and seas, and... intestinal infections. Unfortunately, the peak incidence of infectious intestinal diseases occurs during the warm season. High air humidity, heat, food contaminated with microbes, lack of personal hygiene and violation of food storage rules contribute to the spread of infectious agents. The most common diseases among the population, called intestinal infections, are dysentery and salmonellosis.
What should you know about dysentery? How to protect yourself and your loved ones from this infection? We will talk about this and much more today in this article.
Dysentery is an infectious disease that occurs with intestinal damage and intoxication.
With the light hand of Hippocrates, this infectious disease received the name “dysentery” (from the Greek “dys”, which means “disorder”, and “enteron”, which means “intestines”). In Ancient Rus', the disease was called “bloody womb”, and today the disease is called shigellosis because of the name of the pathogens - Shigella - from a large and “friendly” family of enterobacteria.
Ways of transmission of the disease
The source of intestinal infection is patients with dysentery or bacteria carriers, that is, people who have no manifestations of the disease, but are infectious to others.
The causative agents of this acute intestinal infection enter the body with food, water, through contaminated household items, dishes, toys and unwashed hands.
Infection occurs due to non-compliance with personal hygiene rules - dysentery, typhoid fever, helminthiasis, cholera, salmonellosis and hepatitis A are diseases of “dirty hands”.
You can also become infected with dysentery by swimming in polluted waters.
Quite often the cause of the disease is our carelessness. You finished eating expired yogurt or bought shawarma on the beach - what’s wrong with that? For some it may be nothing, but for others such an experiment with their health may result in treatment.
Dysenteric geography
Bacterial dysentery is more common in European countries, amoebic dysentery - in India and Mexico.
Tourists planning a trip and getting vaccinated against dysentery should not forget about this.
It has been observed that children, adolescents and people with chronic diseases are more susceptible to bacillary dysentery.
Sonne's dysentery is most often caused by dairy products contaminated with bacteria; Flexner's dysentery is transmitted through contaminated water; amoebic dysentery can be “caught” by eating unwashed vegetables, herbs, and contaminated water.
In addition, the causative agent of dysentery is carried by cockroaches and flies.
The disease more often “makes itself known” in the summer-autumn period, since it is at this time that the most favorable conditions are created for the spread of yersiniosis, dysentery and salmonellosis.
Infectious disease doctors warn that the most dangerous dish in the summer is salads dressed with mayonnaise! Almost all foods that have not been heat-treated can pose a health risk - for example, raw eggs, shellfish, sushi, milk, vegetables and herbs.
Characteristics of the pathogen
Sonne's dysentery bacillus is a non-motile microbe, does not form spores, and is not very stable in the external environment. The optimal temperature for its life activity is 370C, but it can reproduce at 150C. Keeps well in water. Shigella sonne is resistant to many antibacterial drugs. When heated to 600C it dies in 10 minutes, and at 1000C it dies instantly. The stick is sensitive to common disinfectants.
The Sonne bacillus has the lowest virulence (ability to infect). But they are characterized by high enzymatic activity and reproduction rate, especially in dairy products, which makes them more dangerous.
So, at room temperature, a dose sufficient to infect an adult accumulates in milk in 8-24 hours. And on a hot summer day, an infectious dose of bacteria for a child accumulates in 1-3 hours. Thanks to its antagonistic activity, Shigella suppresses lactic acid and non-pathogenic microflora.
Forms of dysentery
- bacterial carriage (can be detected accidentally);
- acute dysentery lasts up to three months;
- Chronic dysentery lasts more than three months.
Dysentery in adults, both acute and chronic, can have a mild, moderate or severe course of the disease. In children, signs of dysentery are accompanied by severe intoxication and dehydration.
Acute dysentery
Like any infectious disease, acute dysentery has a certain incubation period, that is, a period of time during which bacteria enter the body and multiply there, as in an incubator. On average, the incubation period can last about 1-2 days.
Most often, acute dysentery occurs with damage to the large intestine, but there are variants of the disease when the stomach and small intestine are involved in the inflammatory process.
After the incubation period, the period of the height of the disease begins - the first symptoms appear. In adults, fever, chills, headache, weakness and drowsiness appear. Each bowel movement is preceded by paroxysmal abdominal pain. The patient notes pain during and after defecation. The feces are liquid, mixed with mucus and blood. During the day there can be up to 100 urges to recover, although the number of bowel movements is small. Concerned about heartbeat, decreased blood pressure, poor appetite.
With inflammation of the upper gastrointestinal tract, nausea, watery diarrhea, and vomiting occur.
Depending on the severity of the disease, this period lasts about a week.
Symptoms in children develop against the background of severe intoxication. Frequent urges to go to the toilet exhaust the child, he is lethargic, refuses food, and cannot swallow liquid. There are signs of severe dehydration: no urination, no sweat, no tears, dry skin and tongue. The baby may complain of chills, abdominal pain, and headache.
Parents need to understand that an insidious infection can cause serious harm to the child’s health. Therefore, when the first manifestations of an intestinal infection appear, it is necessary to urgently call an ambulance or consult a pediatrician. Before the doctors arrive, it is necessary to dehydrate the baby and reduce intoxication by giving him Enterosgel sorbent.
As a result of the treatment, acute manifestations of the disease gradually fade away and recovery occurs. Less commonly, the process becomes chronic.
Chronic dysentery
Chronic dysentery in adults has a relapsing course, as doctors say, that is, it consists of periods of exacerbation and relative well-being. Exacerbation of the disease is caused by seasonal acute infections of the upper respiratory tract and errors in diet. The severity of symptoms during the exacerbation period is less than in the acute form. Intoxication is less pronounced, the body temperature rises to 37.5°C, diarrhea, defecation is less painful, and there is not always blood in the stool.
Chronic dysentery in children and adults can be accompanied by anemia, hypovitaminosis, dysbacteriosis, weight loss, insomnia, and anorexia.
Dysentery in children is often complicated by urinary tract infection, bronchitis and pneumonia.
Do newborns get dysentery?
Unfortunately yes. Children in the first year of life can also develop this disease. The risk group includes:
- premature babies;
- low weight babies;
- with anemia;
- rickets;
- diathesis;
- children who are bottle-fed.
general description
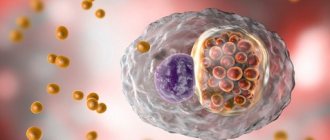
What is a dysentery bacillus? The definition and description of this microorganism can be found in many textbooks on infectious diseases. This bacterium is otherwise called Shigella. It belongs to the Enterobacteriaceae family and is rod-shaped. When stained with Gram stain, Shigella is discolored. Such bacteria are called gram-negative. They have a dense cell membrane and are resistant to antibodies.
Shigella is a non-motile microorganism. Her body does not have flagella or cilia. This bacterium cannot exist in the form of spores and capsules.
According to the method of reproduction, the dysentery bacillus does not differ from most bacteria. New microorganisms are formed as a result of division. Shigella multiplies primarily in the human intestine. However, some varieties of these bacteria can divide while in food.
According to the method of feeding, the dysentery bacillus is classified as a parasite. The bacterium exists at the expense of the human body. Shigella feeds on organic substances produced in the intestines.
Atypical manifestations of dysentery
- erased form of the disease - characterized by minor intestinal symptoms and lack of intoxication, so patients rarely seek medical help;
- fulminant form - severe intoxication, acute renal failure;
- gastroenterocolitic form - its manifestation resembles foodborne toxic infection.
Symptoms and treatment depend on the type of pathogen. Shigella Sonne often causes bacterial carriage and the disease caused by this pathogen occurs in the form of a foodborne toxic infection. Shigella Grigorieva-Shiga causes severe dysentery, with severe intoxication and intestinal symptoms, while Flexner's shigellosis is characterized by a milder course of the disease.
Classification of shigellosis
According to the clinical classification, dysentery is distinguished:
- Spicy:
- with typical (colitic);
- atypical (gastroenteric and gastroenterocolitic) forms.
- Chronic:
- continuous;
- recurrent.
- Bacterial excretion:
- subclinical (without clinical manifestations);
- convalescent (during the recovery period).
What diseases should the disease be differentiated from?
Treatment of dysentery in adults begins after other diseases have been excluded: bacterial and viral intestinal infections, amoebiasis, ulcerative colitis, colon cancer.
With amoebic dysentery (amebiasis), the stool looks like “raspberry jelly”, the disease occurs without severe intoxication and significant fever.
With salmonellosis, bowel movements are not accompanied by painful or false urges, and the feces look like swamp mud.
Cholera is accompanied by profuse diarrhea and dehydration, and the stool has the appearance of rice water. Abdominal pain, fever and false urges are not typical.
With typhoid fever, the liver and spleen are enlarged, and there are rashes on the skin.
With nonspecific ulcerative colitis and colon cancer, there are characteristic changes in the mucous membrane of the large intestine. The diagnosis is established after instrumental examination.
Pathogenesis
For the development of the disease, it is enough for 100 microbial bodies to enter the body. Bacteria produce the following types of toxic substances:
- Endotoxins. They are released only when Shigella is destroyed. Cause general intoxication of the body.
- Enterotoxins. They irritate the intestinal walls and stimulate the formation of fluid and salts.
- Cytotoxins. Destroys intestinal epithelial cells.
- Neurotoxins. This type of poison is produced only by Grigoriev-Shiga bacteria. Toxins affect the central nervous system.
Pathology develops in several stages:
- Bacteria enter the body through the mouth. Then they enter the stomach, where some of the Shigella die under the influence of hydrochloric acid. The destruction of bacteria is accompanied by the active release of endotoxins.
- Surviving dysentery bacilli enter the intestines and release enterotoxins. Poisons act on the walls of the organ and increase the secretion of fluid and electrolytes.
- Bacteria produce cytotoxins and invade epithelial cells. This process is accompanied by the struggle of immune cells against the infectious agent. In this case, some of the Shigella die and release endotoxins.
- The inflammatory process begins in the intestinal walls.
Shigella primarily affects the sigmoid and rectum areas. Bacterial toxins affect not only the lower gastrointestinal tract, but also the heart, blood vessels and adrenal glands. If infection with Grigoriev-Shiga bacteria occurs, the central nervous system is damaged by neurotoxins.
If treatment was carried out in a timely manner, the disease ends in recovery. As already mentioned, even after the symptoms of the pathology disappear, the patient continues to excrete bacteria for some time. In some cases, dysentery becomes chronic.
Currently, thanks to the use of modern antibiotics, the mortality rate for shigellosis has decreased to 5-7%. After an illness, a person does not develop stable immunity, so re-infection is possible.
Treatment
The main principle is the earliest possible start of therapeutic measures.
Treatment of dysentery in children is carried out in the infectious diseases department. Adults with mild forms of the disease can be treated at home, while adults with severe and moderate forms of dysentery are treated in a hospital. What therapeutic measures do doctors use against dysentery?
Medical nutrition
Diet therapy plays an important role. In the acute stage of the inflammatory process, a therapeutic diet low in carbohydrates and fats is prescribed. Patients take food 5-6 times a day in small portions. Foods that cause bloating are not recommended.
Products recommended by nutritionists:
- pureed vegetable soups;
- wheat crackers;
- fish soups;
- omelet, soft-boiled eggs;
- white bread crackers;
- boiled lean meat or fish;
- porridge with water (oatmeal, rice).
Foods that doctors advise to exclude from the diet:
- fatty meats and rich broths;
- flour products;
- fresh bread;
- salted fish;
- sausage;
- pearl barley and millet porridge;
- pasta;
- beans, peas;
- jam, compotes;
- fresh vegetables and fruits;
- milk;
- coffee.
Drug therapy
The main drugs against dysentery are antibiotics. In some cases, a polyvalent bacteriophage is also prescribed. The duration of the course of antibiotics is up to 7 days.
To remove bacterial toxins from the body, patients are prescribed Enterosgel sorbent.
Taking antidiarrheal medications is contraindicated for the patient! These medications slow down the removal of the pathogen from the intestines.
After a course of antibiotic therapy, intestinal dysbiosis is treated and the normal bacterial picture of the intestine is restored. If necessary, vitamins, antihistamines and immunostimulants are prescribed. If food digestion is impaired, digestive enzymes are prescribed.
Comprehensive treatment of dysentery in children includes:
- combating dehydration - drinking plenty of fluids, saline solutions;
- bed rest;
- fight against intoxication (Enterosgel);
- therapeutic diet;
- antibacterial therapy;
- enzymes;
- To reduce intestinal discomfort, Enterosgel is recommended;
- prebiotics and probiotics to restore intestinal microflora.
Children in the recovery stage are prescribed vitamins, decoctions of medicinal herbs, medications that increase the body's defenses, and spa treatment.
Diagnostics
The clinical diagnosis can be confirmed by bacteriological examination of vomit and stool. But the sowing rate of the stick is not high - from 20 to 50% of cases. When Shigella is isolated, its sensitivity to antibacterial drugs is determined.
A serological blood test is also used to detect antibodies to Shigella. But the study requires the collection of paired blood sera taken after the 5th day of illness and with an interval of 5-7 days. Therefore, these studies can only be used for retrospective diagnosis. Express methods can be used to detect antigen using an antibody diagnostic in serological reactions (ELISA, RNGA, RCA, etc.). In particularly severe cases, PCR may be done to detect the antigen in the stool.
Sigmoidoscopy is used in rare cases, for complex differential diagnosis.
Preventive actions
Infection can be prevented by observing basic hygiene. Prevention of dysentery includes:
- washing hands before eating;
- proper storage and adherence to cooking technology;
- mandatory boiling of milk and water before consumption;
- isolation of a patient with dysentery, thorough disinfection of his linen and utensils;
- preventive examination of catering workers to exclude bacteria carriage;
- isolation of sick children, ban on visiting kindergartens and schools until complete recovery and negative stool culture results.
Prevention
To avoid infection with Shigella, you must follow the following recommendations of infectious disease doctors:
- Wash your hands regularly and practice personal hygiene.
- Subject meat and fish to thorough heat treatment.
- Wash vegetables, fruits and berries well.
- Drink only boiled water.
- When swimming in closed reservoirs, avoid accidental swallowing of water.
- Do not use water from ponds for watering garden crops.
- Exercise great caution when in contact with patients with dysentery.
- Eliminate unwanted insects indoors.
The Shigellvac vaccine has now been developed. It prevents infection with Shigella Sonne. A vaccine against Flexner's dysentery is under development. In some cases, dysentery bacteriophage is used for emergency prevention of infection.
However, dysentery does not leave lasting immunity. Therefore, the vaccine is only valid for 12 months. Vaccination is not carried out en masse, but only according to strict indications. It is given to catering workers, medical staff of infectious diseases hospitals and bacteriological laboratories, as well as travelers traveling to dysentery-prone regions.
Complications
From the intestinal side, complications of bacillary dysentery are expressed in the fact that gangrenous lesions of the colon mucosa develop due to a mixed infection. The patient secretes dark, extremely foul-smelling masses, consisting mainly of dead shreds of intestinal mucosa, pus and mucus. With rapid decay, heavy, sometimes fatal bleeding may occur. Another common complication is prolapse of the anal part of the rectum, which can be temporary or permanent. In a temporary case, the rectal mucosa comes out only during tenesmus and, when it stops, it retracts itself again. With constant prolapse, the mucous membrane has to be reduced. Sometimes the fallen parts undergo gangrenescence.
It is not uncommon for convalescents to experience joint damage in the form of so-called dysenteric rheumatism. The joints of the lower extremities are most often affected. Serous exudate is always found in the joint cavity, but bacteriological examination is sterile. At the same time, the tendon sheaths may become inflamed. The process proceeds favorably and passes without a trace.
Suppurative processes caused by secondary infection with pyogenic microbes are also associated with dysentery disease. Purulent parotitis, often leading to septicemia, as well as multiple liver abscesses due to purulent inflammation of the portal vein deserve serious attention. However, the described complications from the liver are rare, which is explained by the low tendency of ulcers to penetrate deeply.
Pathological anatomy
Changes in bacillary dysentery are concentrated almost exclusively in the large intestine, and occasionally the lower part of the small intestine is also involved in the process. The highest degree of damage is found in the rectum and colon; upward they gradually decrease in intensity. It happens that the entire tract of the large intestines is intensively and evenly captured by the process. The essence of the changes comes down to the development of fibrinous inflammation of the intestinal wall.
There are four stages of bacillary dysentery.
• In the first stage, ascertained in mild bacillary dysentery or representing the beginning of severe, swelling of the mucous membrane and round cell infiltration of the submucosal tissue are determined, due to which the intestinal wall is noticeably thickened. The sharp injection of the mucous membrane is striking, especially at the tops of the folds; Numerous hemorrhages are often noticeable. In some places, a grayish pityriasis-like coating can be seen on the surface of the mucosa, as an expression of the beginning necrotization of the epithelium. The process, as observed in mild forms, may not progress, or it may develop and enter the second stage.
• Characteristic of the second stage of bacillary dysentery should be considered rapidly spreading necrosis of the epithelial cover and the sweating of fibrinous exudate on its surface. The latter differs from diphtheria in lower fibrin content and a greater admixture of pus and mucus. In those cases where necrosis does not go deeper than the epithelium, fibrinous deposits have the appearance of delicate, easily removable films. If necrosis penetrates into the depths and covers the entire mucous membrane or even the submucosal layer, then the surface of the intestine appears covered with dirty gray or greenish-gray, with abundant hemorrhages, almost black, dense plaques or, more precisely, scabs. These plaques are formed by fibrinous-purulent exudate and necrotic layers of mucosa located underneath. Muscle layers rarely die, and even more rarely, necrosis reaches the peritoneum. The intestinal wall at this stage thickens even more due to increasing edema and infiltration of the submucosal tissue.
• In the third stage, fibrinous exudate and underlying necrotic tissue undergo purulent melting and separate, and ulcers remain in their place. Ulcerations occupy predominantly the tops of the folds, their edges are infiltrated, and they often have a circular location relative to the intestinal wall. The predominant localization on the folds is explained by the fact that these parts come into closer contact with the contents of the intestine and are more likely to be subjected to its mechanical action. It rarely happens that the ulcer penetrates to the serosa; then, when examining the intestine from the outside, these areas are sharply distinguished by their dark purple color and the presence of a hyperemic belt around the circumference.
• During the recovery stage (fourth stage), the ulcers heal, and with deep defects, flat pigmented scars remain, which in some cases can lead to a narrowing of the intestine.
In severe gangrenous dysentery, necrotic tissue due to the adjoining mixed infection undergoes gangrenous disintegration and turns into a dirty greenish stained mass.
Chronic bacillary dysentery is characterized by the fact that the process seems to freeze in the third stage and the ulcerations do not show a tendency to heal. In a chronic course, the intestinal wall is thickened, its inner surface is pale, the bottom of the ulcers is pale yellowish in color, reaching the submucosal, less often the muscular layer.
Changes in other organs during acute bacillary dysentery, compared with those present in the intestines, are insignificant. In the heart, lesions characteristic of toxic myocarditis are sometimes detected, in the kidneys a picture of nephrosis is observed, nephritis is rare and occurs in later periods of the disease.