Status asthmaticus is a severe complication of bronchial asthma that threatens health. It increases the patient’s risk of death during an attack several times.
The complication is accompanied by constantly developing respiratory failure, with no result from therapeutic measures.
It is extremely difficult to stop an attack in this case. It is important to know the rules of first aid for this condition.
Causes and risk factors
The main causes of status asthmaticus:
- acute or chronic (in the acute phase) infectious and inflammatory diseases of the respiratory system;
- hyposensitizing therapy (aimed at reducing sensitivity to the allergen) during exacerbation of bronchial asthma;
- withdrawal syndrome after a sharp, immediate cessation of glucocorticoid hormones taken for a long time;
- taking medications that can provoke an allergic reaction (salicylates, vaccines, serums, antibacterial drugs, analgesics, etc.);
- massive exposure to allergens;
- incorrect or untimely therapy;
- incorrect assessment of the severity of the condition by the patient himself (at home) or by the attending physician (in a hospital setting);
- “lung locking” syndrome due to an overdose of adrenergic agonists;
- overdose of sleeping pills and sedatives;
- neuropsychic tension, persistent stress.
Triggers of status asthmaticus
First aid for status asthmaticus
During a prolonged asthma attack, you need to know how to properly help the patient.
The emergency care algorithm for status asthmaticus is as follows:
- calling an ambulance. It will not be possible to cope with a protracted attack without qualified medical intervention;
- organization of fresh air flow. It is necessary to open all the windows in the room;
- ensuring the correct position of the patient's body. You need to help him take the correct position: he should sit with support on his hands - this will make breathing somewhat easier. When the correct position is taken, you need to help the victim use the inhaler. Clothing and other items that put pressure on the chest must be removed.
A patient with status asthmaticus should be hospitalized immediately.
After providing first aid, a sign of relief of the patient’s condition is a productive cough. In this case, the airways are cleared of mucus, and breathing is gradually restored.
Symptoms
Each stage of status asthmaticus is characterized by specific symptoms.
Stage I:
- during the day, long-term attacks of suffocation that cannot be controlled by usual medications regularly occur; in the interictal period it is not possible to completely restore breathing;
- painful dry, hacking paroxysmal cough with scanty, viscous glassy sputum;
- forced position of the body, accompanied by shortness of breath (orthopnea) with fixation of the shoulder girdle (the patient sits with his hands resting on the armrests of the chair, or stands leaning against the back of the bed or window sill);
- rapid breathing (up to 40 respiratory movements per minute), involvement of auxiliary muscles in the act of breathing;
- dry wheezing, heard at a distance (distant);
- cyanotic staining of the skin and visible mucous membranes;
- listening during auscultation of the so-called mosaic breathing (in the lower parts of the lungs breathing is not audible, in the upper parts it is hard, with a moderate amount of dry rales);
- pulse is frequent (up to 120 beats per minute), arrhythmic, stabbing, aching pain in the heart area;
- signs of dysfunction of the central nervous system (unmotivated irritability, emotional lability, fear of death, sometimes delusions, hallucinations).
A painful dry cough with scanty sputum indicates stage 1 of status asthmaticus
Stage II is manifested by the following progressive ventilation disorders (extremely severe condition):
- shortness of breath is pronounced, shallow breathing;
- the skin is pale gray, moist;
- forced body position;
- swelling of the veins of the neck;
- liver enlargement;
- the patient's apathy, a state of indifference may periodically give way to agitation;
- Auscultation reveals a “silent lung” (no respiratory sounds are heard over the entire lung or over a large area of both lungs, a small amount of dry wheezing is detected in an isolated area);
- pulse up to 140 beats per minute, weak filling and tension, blood pressure (BP) is reduced, heart sounds are muffled, a gallop rhythm is possible.
At stage III of status asthmaticus, hypercapnic coma develops, its signs:
- disorientation in time and space, the patient is stunned, then loses consciousness;
- the veins of the neck are swollen, the face is puffy;
- diffuse red cyanosis, cold sticky sweat;
- shallow, rare arrhythmic breathing (possibly pathological Cheyne-Stokes breathing);
- during auscultation, respiratory sounds are not heard or are sharply weakened;
- the pulse is threadlike, arrhythmic, blood pressure is sharply reduced or cannot be determined, heart sounds are muffled, and ventricular fibrillation may develop.
Hypercapnic coma develops at stage 3 of status asthmaticus
Classification of status asthmaticus
Status asthmaticus is characterized by impaired breathing during inhalation and prolonged exhalation. When you inhale for a short time, more air enters the lungs than comes out when you exhale, which is caused by blockage and a decrease in the lumen of the airways. Such conditions lead to inflation of the lungs.
Due to an increase in the level of pressure in the chest cavity and inside the alveoli, pulmonary hypertension develops, and the pressure in the cavity of the right ventricle of the heart also increases. In this case, the return of venous blood to the heart is disrupted.
With forced exhalation, the small bronchi undergo even more pronounced spasm. Under such conditions, air stagnates in the lungs, and the amount of oxygen in the blood decreases.
This phenomenon requires immediate hospitalization of the patient.
According to the criterion of occurrence, the following types of asthmatic status are distinguished:
- gradually developing, in which there is a slow increase in mechanical obstruction of the bronchi. The patient has a blockade of beta-adrenergic receptors, receptors that cause constriction of the bronchi are activated;
- anaphylactic. This type of pathology is expressed in an immediate anaphylactic reaction. In this case, mediators of the allergic reaction are released, which is accompanied by total bronchospasm and asphyxia at the time of contact with the allergen;
- anaphylactoid. Reflex bronchospasm occurs as a response to the impact of various irritants on the respiratory tract receptors - physical, mechanical, chemical.
The following stages of status asthmaticus are distinguished:
- relative decompensation;
- decompensation, in which pulmonary function is impaired;
- coma associated with oxygen deficiency.
Any form of status asthmaticus requires urgent qualified assistance.
Diagnostics
Diagnosis of status asthmaticus is based on an analysis of the disease history, clinical manifestations, characteristic auscultatory picture, results of laboratory and instrumental research methods:
- general blood test (for polycythemia, increased hematocrit);
- biochemical blood test (for total protein, protein fractions, seromucoid, fibrin, sialic acids - increased);
- ECG (signs of overload of the right heart are established);
- study of acid-base balance (metabolic acidosis is determined);
- study of the gas composition of the blood (detection of a decrease in oxygen concentration in combination with an increased content of carbon dioxide of varying degrees of severity depending on the stage).
Prevention
It is important for asthmatics to adhere to preventive measures to avoid exacerbation of asthma and the development of status asthmaticus. To do this you need:
- use medications regularly to control asthma;
- always carry with you a medicine that relieves attacks;
- Avoid exposure to food allergens. Chocolate, honey, citrus fruits, nuts, milk, as well as all products with artificial additives - dyes, flavors should be excluded from the daily menu;
- control the intake of sedatives, antihistamines, and sleeping pills;
- limit contact with animals;
- stop smoking, do not go to places with high concentrations of tobacco smoke.
Status asthmaticus is the most dangerous complication of asthma, requiring hospitalization of the patient. Timely treatment can save his life. Without treatment, the patient dies. Under no circumstances should you treat the pathology yourself.
Treatment
The development of status asthmaticus is an urgent pathology and a direct indication for emergency hospitalization.
Mortality from status asthmaticus in out-of-hospital conditions exceeds 70%, in hospital conditions – no more than 10%.
General principles of therapy:
- complete abolition of sympathomimetics with a slowly developing status;
- restoration of sensitivity of beta-adrenergic receptors through the administration of glucocorticosteroid drugs;
- elimination of bronchial obstruction, swelling of the mucous membrane of the bronchial tree, dilution of bronchial secretions;
- correction of blood gas disorders (ventilation, oxygen therapy);
- elimination of decompensated metabolic acidosis;
- infusion therapy to replenish the volume of circulating blood, extracellular fluid, and eliminate hemoconcentration;
- correction of symptomatic changes in blood pressure (hypo- or hypertension);
- combating acute right ventricular failure;
- improving blood rheology, preventing the possible development of thromboembolic disorders;
- fight against foci of bronchopulmonary infection (if necessary).
Oxygen therapy corrects blood gas disturbances in status asthmaticus
The main clinical sign of the effectiveness of the therapy is the appearance of a productive cough with the release of a large amount of viscous glassy sputum, which is then replaced by liquid sputum.
general description
Status asthmaticus (asthmatic condition) is a severe and prolonged attack of suffocation, usually lasting at least 2 hours and not relieved by the medications that the patient usually uses.
The asthmatic condition differs from a regular attack of bronchial asthma in that, occurring in a more severe form, it leads to serious disturbances in the functioning of the respiratory system, heart and nervous system. The fundamental difference between an asthmatic state and an attack of suffocation is that in an asthmatic state, the deterioration of air flow through the bronchi is caused by blockage of their lumen with viscous, glassy, difficult to separate sputum, and during an attack of suffocation - by a spasm of the smooth muscles of the small bronchi. Blockage of the bronchial tree with viscous mucus, overstretching of the alveoli with air, and deterioration of gas exchange in the lungs lead to disruption of the oxygen supply to all vital systems of the body, which leads to significant changes in their functioning, primarily in the brain. Oxygen starvation of the brain leads to various forms of impaired consciousness, including coma. The asthmatic condition is the cause of death in approximately 7% of patients.
The following factors contribute to the occurrence of status asthmaticus:
- Massive exposure to allergic agents.
- Diseases of the bronchopulmonary system of infectious etiology.
- As a rule, excessive use of β2-agonists, incorrectly selected dose of systemic glucocorticosteroids, allergies to certain medications.
Status asthmaticus occurs in patients who have had asthma for a long time and are receiving anti-asthmatic therapy.
Complications
If treatment is ineffective or absent, airway obstruction and oxygen deprivation progress. Status asthmaticus is dangerous because it provokes numerous complications. Among them:
- adrenal insufficiency;
- serious heart rhythm disturbances;
- addition of a secondary infection;
- bleeding of the gastrointestinal tract;
- myocardial infarction;
- hypoxic damage to the central nervous system;
- pneumothorax;
- collapse;
- pulmonary edema;
- coma, death.
Laryngospasm
This is a sudden pathological closure of the vocal cords, which is manifested by a sharp difficulty or inability to inhale. Laryngospasm occurs as a result of a pathological reflex with excessive irritation of the branches of the vagus nerve.
The cause of laryngospasm is traumatic manipulations and operations in the area of reflexogenic zones (vocal cords, tracheal bifurcation, epiglottis, eyeballs, mesentery of the peritoneum, rectal sphincter, periosteum). Irritation of the vocal cords when droplets of saliva, food particles, acidic gastric contents, water, chemical (acid vapors) and thermal (open flame) irritants come into contact with them, an allergic reaction in patients, especially vagotonics, are common causes of laryngospasm.
Laryngospasm can be partial or complete. In both cases, it manifests itself as the sudden onset of inspiratory suffocation. The patient strives to inhale: the respiratory muscles actively contract, the intercostal spaces, the jugular notch, and the supraclavicular fossa are retracted. With partial laryngospasm, a small amount of air penetrates through loosely compressed vocal cords, which oscillate, causing a sound reminiscent of the crowing of a rooster. Total laryngospasm is characterized by aphonia. Within a few minutes, the patient develops cyanosis, tachycardia, and blood pressure increases; later, under the influence of hypoxia, consciousness is lost and reflexes are suppressed. In some cases, relaxation of the striated muscles of the larynx occurs, which leads to the spontaneous elimination of laryngospasm. However, deep hypoxia and hypercapnia can cause circulatory arrest.
Urgent Care:
- establish an oxygenation system through a breathing apparatus mask, since increasing hypoxia worsens the patient’s condition and contributes to the transition of partial laryngospasm to total;
- immediately stop the effect of the stimulus on the reflexogenic zone (if an operation is being performed, stop it);
- Inject the patient intravenously with solutions of atropine sulfate (at the rate of 0.01 mg/kg body weight), aminophylline (2.4% - 5-10 ml, diluted by half with sodium chloride solution). If there is an allergy, chemical or thermal damage to the vocal cords, administer solutions of antihistamines (2.5% pipolfen solution - 2 ml) and glucocorticoids (prednisolone solution 60 - 90 mg).
Specialized assistance:
• inhalation of bronchodilators (salbutamol);
• re-introduction of the above-mentioned mediators;
• in case of partial laryngospasm, perform artificial ventilation of the lungs with large volumes of oxygen through a breathing apparatus mask;
• if there is no effect from the previous treatment, inject intravenously depolarizing muscle relaxants (2% ditilin solution - 10 ml), and, after waiting for complete muscle relaxation, intubate the patient under the control of direct laryngoscopy (it is advisable to first turn off consciousness using, for example, the introduction of p -on ketamine);
• in the absence of conditions for tracheal intubation and a threat to life occurs (severe bradycardia, fainting, a decrease in blood pressure of more than 70 mm Hg, the appearance of generalized convulsions), it is necessary to immediately perform a conicotomy and pump oxygen through a tube inserted into the trachea;
• when diagnosing clinical death, immediately perform cardiopulmonary resuscitation according to generally accepted rules.
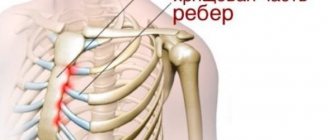
Traumatic chest injuries
Numerous rib fractures, especially fenestrated ones, lead to disruption of the biomechanics of breathing. Clinically, one can observe a decrease in the excursion of the chest, the retraction of its individual parts and asymmetric movements during breathing. Patients experience a decrease in tidal volume, cyanosis of the skin and mucous membranes, destabilization of central hemodynamics, impaired microcirculation, and disorders of consciousness.
Rib fractures may be accompanied by hemo- or pneumothorax. One of the most serious complications is tension pneumothorax, in which hypoxia is severe and displacement of the mediastinal organs can quickly lead to the death of the patient.
In such patients, a medical worker must carry out examination methods available to him: external examination, palpation, auscultation of the lungs and their percussion; laboratory and instrumental diagnostics. Patients delivered in an unconscious state deserve special attention.
Bronchiolospasm
This is an acute violation of the function of external respiration, caused by the closure of the smooth muscles of the small bronchi. It can be partial or complete. The causes of bronchiolospasm and its drug treatment are the same as for laryngospasm. However, the introduction of muscle relaxants does not eliminate bronchiolospasm, and conicotomy is also ineffective. With total bronchial spasm, death, unfortunately, is almost inevitable.
When carrying out manipulations on reflexogenic zones, it is very important to use preventive premedication with the administration of peripheral M-anticholinergics (atropine sulfate solution at the rate of 0.01 mg/kg). This will prevent overexcitation of the parasympathetic nervous system and the occurrence of pathological reflexes.