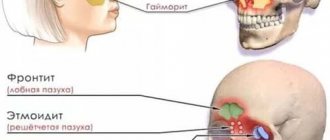
The ENT organs, being an outpost of the immune system on the path of infection into the body, are the first to encounter the effects of various pathogens. That is why inflammatory processes often begin in them. Inflammation of the paranasal sinuses is called sinusitis. In total, a person has 4 pairs of paranasal sinuses, these are cavities filled with air. As a result of inflammatory processes, pus is formed in the sinuses, and the person begins to feel weak and unwell.
1
Nasal endoscopy in MedicCity
2 Nasal endoscopy in MedicCity
3 Rhinoscopy in MedicCity
Causes of maxillary sinusitis –
The main causes of the development of maxillary sinusitis can be divided into 3 groups (in descending order):
- acute and chronic inflammatory diseases of the nose,
- foci of inflammation at the roots of the upper teeth,
- fractures of the upper jaw and zygomatic bone.
Most often, the development of maxillary sinusitis occurs against the background of a runny nose during acute infectious diseases (for example, ARVI and influenza), as well as against the background of chronic rhinitis.
These causes account for about 62% of all cases of the disease. In this case, most often inflammation occurs in the presence of predisposing factors, for example, a deviated nasal septum, obstruction of the nasal passages, or against the background of allergic rhinitis or polypous growths in the nasal passages. An equally important role is played by the patency of the anastomosis connecting the maxillary sinuses with the nasal cavity, through which the process of physiological cleansing of the sinuses occurs. The second large group of causes are causes of odontogenic origin (i.e., related to teeth). In approximately 32% of cases, the development of maxillary sinusitis is associated with inflammatory foci at the apexes of the roots of the 5-6-7 teeth of the upper jaw. The fact is that the bottom of the maxillary sinuses is located only 1-3 mm from the apexes of the roots of these teeth, and therefore, if a focus of inflammation occurs at the apex of the root, the inflammation can also affect the mucous membrane of the sinuses (Fig. 5).
Odontogenic maxillary sinusitis can also develop - 1) due to errors in filling root canals, when the filling material is removed beyond the apex of the root, 2) as a result of pushing the infected pulp beyond the apex of the root during the treatment of pulpitis and periodontitis, 3) when perforation of the maxillary sinus occurs, caused by time of removal of the lateral teeth of the upper jaw, 4) as a complication during implantation of teeth in the lateral parts of the upper jaw.
Important: a large group of patients may simultaneously have both rhinogenic and odontogenic causes of sinusitis.
For example, in the area of the apex of the roots of the 5-6-7 upper teeth, the patient may have foci of chronic inflammation, which in themselves did not cause inflammation of the mucous membrane of the maxillary sinuses. But in the case of the development of ARVI, not only an acute runny nose develops (which makes it difficult for the mucous secretion to drain from the maxillary sinuses), but also the activation of inflammatory foci in the area of the apexes of the roots of the teeth. The combination of these factors greatly increases the risk of developing sinusitis in a patient.
Features of the disease in children
The clinical picture of acute sinusitis in children varies depending on age, origin, location, and the presence of concomitant pathology.
In childhood, the ethmoid sinus is affected more often (about 80% of all sinusitis cases) than in adults. The second place in this age group is occupied by inflammation of the maxillary sinus. The presence of a common bone wall and the close location of the excretory ostia causes frequent combined lesions of these sinuses. Frontal sinusitis occurs less frequently in children over 6-7 years of age, which is associated with the formation of the frontal sinus. The sphenoid sinus is rarely affected in children.
In the general structure of ENT pathologies in childhood, sinusitis accounts for approximately 32%.
In newborns, as well as in infants and young children, acute sinusitis is more severe, and general symptoms prevail over local ones. In addition, in children of this age group, acute sinusitis can imitate the clinical picture of other pathologies (lower respiratory tract and even gastrointestinal tract, due to the severity of intoxication).
In a mild form of the disease, the general condition is within normal limits, the temperature rises to low-grade levels or remains within normal limits. The headache is not too intense and not constant. Local signs of the inflammatory process are moderately expressed.
In the moderate form, signs of general intoxication of the body, as well as local inflammatory changes, are more pronounced.
A severe course is characteristic of poly- or pansinusitis, especially with the development of orbital and intracranial complications. The child’s general condition deteriorates sharply, with severe headache, pain in the affected sinus and orbit, photophobia and lacrimation. The temperature is usually high (38 °C and above).
Acute sinusitis -
As we said above, acute sinusitis can be rhinogenic or odontogenic. In the first case, it will develop against the background of acute respiratory viral infections and influenza, chronic nasal diseases, and allergic rhinitis. And in this case, the development of sinus inflammation occurs against the background of a runny nose, nasal congestion, and the development of swelling of the mucous membrane of the nasal passages. The fact is that swelling of the mucous membrane leads to a narrowing or complete closure of the openings between the maxillary sinuses and the nasal cavity, which leads to disruption of the outflow of mucous secretion from the sinus and serous exudate formed during inflammation.
If the development of sinusitis is associated with teeth, very often patients complain of pain in one of the lateral teeth of the upper jaw, which preceded the onset of sinusitis. In some patients, the pain may be sharp and throbbing, while in others it appears only when biting on the causative tooth. Some patients may experience only slight discomfort in one tooth, but in some cases there may be no toothache at all (in which case the causative tooth can only be identified through an x-ray). In such patients, sinusitis does not develop against the background of a runny nose and nasal congestion, and nasal discharge appears only later.
At the first stage of the development of sinusitis - in addition to a runny nose and nasal congestion with rhinogenic sinusitis, or pain in one of the teeth with odontogenic sinusitis - the patient is usually initially only bothered by malaise. In the initial period, the inflammation is serous in nature and the formation of pus in the sinus does not yet occur. Mucous discharge from the nose during this period still has a transparent color, without an unpleasant odor. In general, the patient does not present any active complaints at the initial stage, but everything changes when serous sinusitis gradually turns into purulent sinusitis.
Symptoms during the transition of serous sinusitis to purulent:
- Purulent exudate may be released from the nasal passage on the side of the inflamed maxillary sinus, the discharge of which may intensify when the head is tilted forward (Fig. 7). In the morning, you can often notice traces of pus leaking from the nose on the pillow. But if the outflow of purulent exudate from the sinus into the nasal cavity is completely disrupted, then such a symptom may be absent.
- A feeling of heaviness may appear in the corresponding half of the face, which is typical if only one maxillary sinus is inflamed.
- When pressing on the skin in the projection of the anterior wall of the sinus, pain may be felt. In addition, pain or discomfort may be felt when tapping on the teeth located in the projection of the inflamed sinus (usually the 5-6-7 teeth of the upper jaw).
- Common symptoms include lethargy, weakened sense of smell, chills, loss of appetite, and weakness.
- Body temperature can rise to 37.5 - 39.0 degrees (sometimes higher).
- Increasing pain, which is initially localized in the projection of the inflamed sinus, but then can spread to the frontal, temporal, occipital regions, and to the area of the upper jaw teeth.
- With severe sinusitis, swelling of the soft tissues of the face may also be observed due to their edema, redness, as well as the development of purulent purulent periostitis from the oral cavity.
Computed tomography and radiography –
The final diagnosis is made based on the symptoms of maxillary sinusitis and data from computed tomography or radiography. It is optimal to do a computed tomography (CT) scan, because Such photographs will allow not only to examine the sinuses in different projections, but also to simultaneously inspect all the teeth of the upper jaw - for the presence of inflammatory foci and poorly filled root canals. The latter is very important for establishing the cause of sinusitis and choosing the right treatment tactics (24stoma.ru).
At the end of the article, we will present a specific clinical case in which the patient was mistakenly diagnosed with maxillary sinusitis of rhinogenic origin. As a result, she was tormented for several years with punctures, rinses, and antibiotics, while she had classic odontogenic sinusitis (the cause of which was a focus of inflammation at the apex of the root of one of the teeth in the upper jaw). Therefore, it is very important to conduct a full diagnosis and establish the correct cause of the disease.
CT scan of the paranasal sinuses (normal and pathological) –
An important feature of CT is that it allows you to visualize not only the filling of the sinus with pus. For example, with chronic maxillary sinusitis, there may be no pus in the sinus at all, and the process develops like catarrhal inflammation (hyperplastic thickening of the sinus mucosa). In this case, CT allows us to consider in which areas of the mucous membrane in the sinus changes occur. For example, if we see changes in the area of the bottom of the sinus, we immediately assume that the inflammation is associated with the teeth.
If the mucous membrane is thickened primarily in the area of the anastomosis with the nasal passages, then first of all we assume that the inflammation is of a rhinogenic nature (i.e., the infection has spread from the nasal cavity). As for traditional radiography, it is much less informative and only allows one to judge the presence of inflammation in it by the degree of darkening of the sinus, as well as see the level of pus in the sinus.
Acute purulent sinusitis on x-ray –
Forms of the disease
Depending on the localization of the pathological process (damage to one or another sinus), acute sinusitis is divided into:
- sinusitis - inflammation of the maxillary sinus;
- frontal sinusitis - inflammation of the frontal sinus;
- sphenoiditis – inflammation of the sphenoid sinus;
- ethmoiditis - inflammation of the ethmoid labyrinth.
The development of intracranial complications of acute sinusitis can cause death.
The disease can be unilateral or bilateral, complicated or uncomplicated, one (monosinusitis), several (polysinusitis) or all (pansinusitis) paranasal sinuses can be affected.
Types of sinusitis
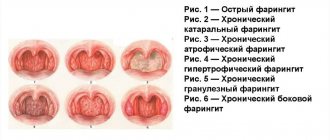
Depending on the nature of the inflammation, acute sinusitis is classified into catarrhal (serous), purulent, hemorrhagic, necrotic.
Depending on the severity of clinical manifestations, the course of the disease can be mild, moderate or severe.
Chronic sinusitis: symptoms
Acute maxillary sinusitis in adults, in the absence or improper treatment, can very quickly become chronic. If you have developed chronic sinusitis, the symptoms in adults depend on the form of chronic inflammation, which can be either catarrhal, or purulent, or polyposis, or purulent-polyposis.
- Catarrhal form - this form is usually practically asymptomatic, but with periodic, not pronounced exacerbation of the inflammatory process.
During exacerbations, patients may complain of a feeling of heaviness in a certain half of the face (due to the inflammatory process), periodic disruption of nasal breathing, as well as some malaise at the end of the day. During an instrumental examination of the nasal passages, the ENT doctor can detect swelling and cyanosis of their mucous membrane. X-rays for this form of sinusitis usually do not give results at all, but a CT scan may show thickening of certain areas of the mucous membrane in the sinus (in areas of inflammation). You can see the catarrhal form of sinusitis in the CT image in Fig. 9 - in the sinus (on the left in the image) you can see a thickening of the mucous membrane in the area of the bottom of the sinus, as well as the wall adjacent to the nasal passages.
- Purulent and polypous forms - the diagnosis of chronic sinusitis is made based on symptoms and X-ray or CT data, as well as endoscopic sinusoscopy. In the purulent form, the sinus will be partially filled with purulent exudate, and in the polypous form, there will be growths of polyps on the surface of the mucous membrane (a combined purulent-polypous form of sinusitis may also occur). Polyps in the maxillary sinus are no different from polyps that often grow in the nasal passages, and they look the same (Fig. 12).
Patients with purulent and polypous forms of chronic sinusitis usually present the following complaints:
→ fatigue, → putrid odor, → periodic discharge of pus from the corresponding half of the nose, → temperature 37.5 – 37.8.
Chronic sinusitis in the acute phase -
If the source of inflammation of the sinus mucosa has not been eliminated, or improper treatment or self-medication has been carried out, the acute inflammatory process becomes chronic, which in turn is characterized by a wave-like course. The latter means that periods of remission will periodically be replaced by exacerbations (a wave-like course of inflammation). Exacerbations of chronic sinusitis can occur for various reasons, for example, against the background of hypothermia or decreased immunity, against the background of acute respiratory viral infections, exacerbation of chronic inflammation in the area of the apexes of the roots of 5-6-7 teeth, etc.
Chronic sinusitis in the acute phase is characterized by symptoms similar to acute maxillary sinusitis, which we described above. Very often, the development of chronic sinusitis is a complication of incorrect actions by the doctor, or when the patient is addicted to self-medication. Below I will demonstrate an example from my own clinical practice.
Ethmoiditis
Ethmoiditis is an acute or chronic inflammation of the mucous membrane of the cells of the ethmoid labyrinth (anatomical labyrinth in the bridge of the nose). Ethmoiditis is bacterial or viral in nature.
There are acute and chronic ethmoiditis. Acute ethmoiditis accompanies influenza, rhinitis and is complemented by inflammation of the paranasal sinuses.
Ethmoiditis in adults affects both the frontal and maxillary cavities. With weak immunity, the acute form of ethmoiditis turns into long-term chronic ethmoiditis with periods of exacerbation and remission.
Polypous ethmoiditis is characterized by the appearance of polyps in the mucous membrane of the ethmoid labyrinth of the forehead. Polypous ethmoiditis may appear after chronic, allergic rhinitis.
Catarrhal ethmoiditis occurs due to the activity of viruses. It is characterized by increased lacrimation, weakness, nausea, dizziness, swelling in the bridge of the nose, and fever.
Ethmoiditis in children is a very serious disease. The infection spreads very quickly due to the anatomical structure of the ethmoid labyrinth. The development of ethmoiditis in children requires urgent hospitalization.
Symptoms of ethmoiditis
Acute catarrhal ethmoiditis. Symptoms
- pain in the bridge of the nose and at the wings of the nose;
- heavy breathing through the nose;
- loss of smell;
- headache, weakness;
- profuse nasal discharge, which gradually becomes purulent;
- temperature rises to 38 degrees;
- In children, the inner corner of the eye socket also swells and turns red.
In the acute form, primary and secondary ethmoiditis are distinguished.
With primary ethmoiditis, anxiety, vomiting, dyspepsia and toxicosis appear, the temperature is 39-40 degrees.
Secondary ethmoiditis is more severe and develops faster. The patient is in extremely serious condition with pronounced septic symptoms. The eyelids become swollen and cyanotic, swelling of the conjunctiva and noticeable protrusion of the eyeball are observed, and nasal breathing becomes difficult.
Chronic ethmoiditis. Symptoms
- headaches that are difficult to register by localization;
- weakness, rapid fatigue of the patient;
- soreness in the bridge of the nose when pressed and painful points at the wings of the nose;
- purulent discharge with a nauseating odor;
- extensive mucus in the nasopharynx, which is difficult to spit out;
- emerging polyps.
Complications after ethmoiditis:
- meningitis;
- encephalitis,
- intraocular and intracranial pressure;
- destruction of the ethmoid bone.
Treatment of ethmoiditis
Treatment of ethmoiditis in acute form is predominantly conservative. It is necessary to ensure the outflow of mucus with the help of vasoconstrictors and physiotherapeutic procedures.
Treatment of ethmoiditis in chronic form is predominantly surgical.
1 MRI in MedicCity
2 Laboratory diagnostics in MedicCity
3 Ultrasound examination of the paranasal sinuses in MedicCity
Maxillary sinusitis: treatment
Treatment of maxillary sinusitis begins with establishing the cause of its occurrence, and this is the most important stage in treatment. You probably already realized that if sinusitis is associated with teeth (odontogenic origin), the treatment should be completely different than if the cause was an infection in the nasal cavity (rhinogenic origin). Plus, you should know that there are also combined causes that aggravate each other.
With the causes of rhinogenic origin, everything is basically clear here - these are acute and chronic inflammatory processes in the nasal passages, occurring with acute runny nose and/or nasal congestion, etc. But the dental causes of maxillary sinusitis are more interesting. Firstly, there are poorly filled root canals in the area of 5-6-7 teeth and foci of inflammation at the apexes of the roots of these teeth. Secondly, the cause of sinusitis can be filling material that is abundantly removed beyond the apexes of the roots (when filling root canals).
Thirdly, sinusitis can occur as a result of traumatic removal of 5-6-7-8 teeth. For example, the doctor may push a fragment of tooth or bone tissue into the sinus. Or he can simply make a perforation (a hole through the sinus) with an instrument. According to the rules, after this the doctor must perform gum surgery to tightly sutured the extraction site, but in fact, 95% of dental surgeons simply do not do this. As a result, a fistula is formed between the oral cavity and the sinus, and infection from the oral cavity penetrates into the sinus, causing inflammation in it. Next we will talk about how to treat sinusitis.
Frontit
Frontal sinusitis (frontal sinusitis) is an inflammatory disease of the frontal paranasal sinus. This type of sinusitis is the most severe. There are forms of acute and chronic frontal sinusitis.
Symptoms of sinusitis
Acute frontal sinusitis, symptoms:
- pain and swelling around the nose and eyes;
- increased pain when tapping in the projection area of the inflamed sinuses;
- heavy breathing due to inflammation of the nasal passages;
- runny nose with thick yellow or green mucus;
- increase in body temperature to 38-39 degrees;
- severe headache (minor relief occurs when lying down);
- pain radiating to the ears and teeth;
- fear of light;
- severe weakness;
- sometimes sore throat, difficulty identifying odors, decreased pungency of taste.
Chronic frontal sinusitis, symptoms:
- aching headache;
- purulent, unpleasant-smelling nasal discharge in the morning;
- slight increase in temperature;
- difficulty breathing through the nose;
- sputum discharge in the morning.
Causes of frontal sinusitis
The following reasons for the development of frontal sinusitis are distinguished:
- viral, bacterial or fungal infection;
- complication after influenza, ARVI, etc.;
- getting foreign objects into the nose;
- long-term infectious or allergic rhinitis (rhinitis);
- deviated nasal septum;
- adenoids;
- allergy;
- nasal polyps.
Treatment of frontal sinusitis
How to treat frontal sinusitis? Definitely under the supervision of an otolaryngologist! The disease is not only difficult for many patients to tolerate, but also has dangerous complications, including orbital abscess, meningitis, sepsis, etc.
Treatment of sinusitis is aimed at eliminating infection in the sinuses and stopping inflammation. Medicines will help relieve swelling, improve ventilation of the sinuses and lead to the discharge of contents from them. If the disease is viral in nature, then antibiotics for frontal sinusitis are mandatory!
The following antibiotics are used to treat sinusitis:
- penicillin antibiotics (semi-synthetic or synthetic amoxicillin preparations);
- cephalosporin antibiotics;
- macrolide antibiotics (they do not affect the intestinal microflora);
- local antibiotics in the form of nasal drops, nasal spray, aerosol;
- homeopathic medicines;
- symptomatic remedies for frontal sinusitis in the form of vasoconstrictor nasal drops, antipyretics and anti-inflammatory drugs.
In case of severe frontal sinusitis and insufficient effectiveness of conservative treatment, sinus lavage using the method of displacement and puncture is prescribed.
1 Rhinoscopy in MedicCity
2 Consultation with an ENT specialist in MedicCity
3 ENT consultation in MedicCity
Prevention of frontal sinusitis
To prevent frontal sinusitis, you need to monitor the state of your immune system, promptly eliminate foci of inflammation in the ENT organs, harden your body, and lead a healthy lifestyle.
Treatment of acute sinusitis –
Acute maxillary sinusitis of rhinogenic origin can be cured without the use of antibiotics, but only if you consult a doctor at the very beginning of the development of inflammation (until serous inflammation turns into purulent). The most important thing at this stage is to relieve swelling of the nasal mucosa, because the edematous mucous membrane increases in volume and blocks the anastomosis between the maxillary sinus and the nasal cavity. Removing edema will normalize the outflow of serous inflammatory exudate from the sinus.
Traditional sprays for the common cold can be used for no more than 2-3 days, because their longer use leads to the opposite effect - persistent swelling of the mucous membrane. Therefore, in order to quickly relieve swelling of the nasal mucosa, it is better to use such remedies only during the first 2 days. An exception may be the spray for runny nose “Rinofluimucil”, which can be used for up to 7 days. This drug not only relieves swelling of the nasal mucosa, but also reduces the viscosity of mucopurulent discharge (i.e., it will improve the outflow from the sinuses).
After eliminating acute symptoms, it is better to switch to the drug “Nasonex” (spray), which contains low dosages of glucocorticoids that do not have a systemic effect. This drug has a pronounced anti-inflammatory, anti-allergic and anti-edematous effect, and is used for up to 3 weeks. In addition, the doctor may additionally prescribe you herbal preparations “Sinupret”, “Sinuforte”, “GeloMyrtol Forte” (they stimulate the removal of inflammatory exudate from the sinuses). However, they can only be used when the outflow of exudate from the sinus is not impaired.
Drugs for the treatment of sinusitis in adults -
If the serous process has turned purulent, then there are all indications for antibiotic therapy, as well as for rinsing the sinuses through the nose. For lavage, it is better to use the YAMIK sinus catheter - today this is the best and most effective option. And if the clinic doesn’t use it, but does traditional punctures, then this is not a serious clinic at all and it’s better to run away from there. How to choose a good clinic: serious ENT clinics always perform endoscopic maxillary sinusotomy using a shaver, and sinus lavage is carried out only using a Yamik sinus catheter.
Antibiotic therapy for sinusitis -
Antibiotics of choice for the treatment of sinusitis:
- β-lactam lactamase-protected synthetic penicillins (amoxicillin + clavulanic acid, or ampicillin + sulbactam, or piperacillin + tazobactam, or cefoperazone + sulbactam, or ticarcillin + clavulanic acid), or carbapenems (imipenem or meropenem).
- Macrolides (azithromycin, clarithromycin).
- Modern fluoroquinolones (levofloxacin or moxifloxacin).
- III-IV generation cephalosporins (ceftriaxone or cefepime).
- Oxazolidones (linezolid) – only when multi-resistant microflora are isolated.
When treating mild to moderate forms of sinusitis, it is better to start treatment with β-lactam lactamase-protected synthetic penicillins. The best option would be a combination of amoxicillin with clavulanic acid, for example, tablet preparations such as Augmentin, Amoxiclav and others. But in severe cases, it is worth choosing either from modern fluoroquinolones, or one of the III-IV generation cephalosporins (but all these drugs in severe cases should already be administered parenterally).
If the patient is intolerant to penicillins - in mild and moderate forms of the disease, we prescribe, for example, macrolide antibiotics or fluoroquinolones (in tablets), and in severe forms - some of the fluoroquinolones (parenterally). And we remember that if you are intolerant to penicillins, you cannot prescribe antibiotics from the cephalosporin group. It is also worth considering that with long-term chronic sinusitis, fungal flora can often join the bacterial infection and, therefore, such patients should be additionally prescribed antifungal drugs (after culture for microflora).
The total duration of antibiotic use usually ranges from 7 to 10 days, but in some cases up to 14 days. We sincerely advise you never, under any circumstances, use Russian-made antibiotics (unless you want to find out what pseudomembranous colitis is). It is also worth considering that the effectiveness of antibacterial therapy increases significantly when, in parallel with the patient, procedures for washing the sinuses with antiseptics are carried out (for example, using the Yamik sinus catheter).
Important: do not forget that if acute sinusitis is associated with the formation of inflammatory foci at the apexes of the roots of 5-6-7 teeth, then at the same time you urgently need to contact a dentist-therapist to open the causative tooth and disinfect the root canals in it using drugs for based on calcium hydroxide (the drug is placed in the root canals for about 1 month). Keep in mind that if sinusitis is odontogenic in nature, then antibiotic therapy without sanitizing the source of infection in the root canals will be ineffective.
And I would like to say a few words separately to patients who are planning to cure their sinusitis at home, using available means, for example, regular nasal rinses and taking antibiotics. In essence, this is useless, although it can lead to short-term improvement, plus it will cause the process to become chronic and require surgical treatment in the future.
How many days does it take to treat sinusitis and how to understand that it is going away - Your online doctor
Symptoms indicating a cold are rarely noticed. If a runny nose starts, it is unlikely that a person will immediately go to the doctor. People usually think that a runny nose will go away on its own. It seems that there is nothing complicated here.
However, what can happen is not simple rhinitis, but quite dangerous sinusitis. He will definitely require consultation with a professional and further serious treatment.
At the same time, you need to know how to recognize sinusitis so that you can do it yourself and seek medical help in time.
Description
Sinusitis is an infectious inflammation of the upper nasal sinuses. It can also occur as a consequence of a deviated nasal septum. The disease cannot be ruled out due to an allergic reaction.
Causes
There are many factors influencing the onset of the disease. Most often it appears as a result of untreated acute rhinitis. Another equally common reason is the use of medications without consulting a doctor.
Other causes of the disease are:
- recurrent inflammatory processes in the upper respiratory tract;
- pathologies in the maxillary sinuses;
- hypothermia of the body;
- chronic rhinitis;
- nasal cavity injuries;
- chronic inflammatory phenomena;
- anatomical disorders of the nose.
Despite such a variety of causes, the disease most often appears in people with a weakened immune system.
When sinusitis begins, the science of psychosomatics usually notes the following reasons:
- constant weakness;
- depression;
- dissatisfaction with the surrounding life;
- low self-esteem;
- state of anxiety.
Thus, psychosomatic signs indicate that the disease is provoked by a lack of care and attention to the person.
Main symptoms
To determine the disease, you need to know how sinusitis manifests itself. The main symptoms are:
- difficulty breathing through the nose;
- pressure is felt from above the bridge of the nose;
- temperature increase;
- loss of smell;
- discomfort when being in the light;
- pain in the temples and forehead;
- swelling of the face;
- pus in nasal discharge.
Here we can note one feature of the disease, which will tell you how to distinguish sinusitis from a runny nose: this is pus in the snot. With ordinary rhinitis, the nose is no less stuffy, but the discharge is different.
How to determine sinusitis yourself
The initial stage of sinusitis is very similar to ordinary rhinitis. It's difficult to notice anything unusual. To understand how to identify sinusitis, you need to pay attention to some signs.
After some time, the patient begins to feel pain when turning his head or bending over. Pain symptoms are also present near the temples and in the frontal sinus. It is characteristic that they become especially strong in the evening. In the morning they are not so depressing.
You should also pay attention to headaches. The disease is often accompanied by migraine. Pain may also be felt in the upper jaw area.
Among other signs by which a common runny nose or sinusitis can be identified are poor appetite and loss of performance. The voice also becomes slightly nasal. With the further development of the disease, the nasal discharge becomes dark brown in color and contains pus. There may also be bloody discharge.
How else can you tell if you have sinusitis? This is indicated by a constant headache, and when blowing your nose, a sensation of shooting pain appears.
Determining the type of sinusitis
There are two types of sinusitis: acute and chronic.
The acute stage is characterized by headaches, a feeling of pressure in the forehead and upper jaw, and purulent nasal discharge. Also for this type of disease, a symptom is high temperature (above 38 degrees). There is general weakness.
As sinusitis develops, the pain increases, the pain is no longer localized, but radiates to the entire facial part. Often the patient cannot even determine where exactly it hurts.
Chronic sinusitis does not have such severe symptoms as acute sinusitis. The pain is not so acute, it is periodic. In the morning, the patient's eyelids become swollen. The nose is constantly stuffy. an increase in temperature is recorded, but it is below 38. The general condition of the body worsens: performance decreases, problems with memory are possible.
Clinical diagnosis of sinusitis
To determine whether you have sinusitis, just a certain set of symptoms is not enough. To make a correct diagnosis, you need to go to a clinic, where the doctor will prescribe a series of diagnostic procedures.
First of all, the doctor will conduct an individual examination using special instruments. If the mucous membrane in the maxillary sinuses is swollen and red, then this is one of the signs of sinusitis.
Next, bacterial culture of the mucus is carried out. With its help, the microflora of secretions is determined. You can find out the cause of the disease in order to prescribe the correct treatment option.
An important diagnostic step is x-ray. Sinusitis is clearly visible in such photographs. Darkened areas in the sinuses are clearly visible, the level of filling with pus is visible. If there is any doubt about the exact diagnosis, they also resort to computed tomography and magnetic resonance imaging.
It is possible to determine sinusitis by puncturing the sinuses. Sometimes this is a therapeutic procedure. But in addition to this purpose, the puncture helps with diagnosis: it is possible to take material for analysis.
Diagnosis of sinusitis in children
The peculiarity of the child’s body is that the maxillary sinuses are not yet fully developed. The child’s immune system successfully copes with this disease. However, at school age the risk of the disease increases. Sinusitis can be a consequence of incompletely treated viral diseases, colds, stomatitis, scarlet fever. Polyps may also be the cause.
Symptoms in children are similar to those of the disease in adults. It can be:
- difficulty breathing through the nose;
- regular runny nose;
- enlarged adenoids;
- regular cough at night;
- swelling of the mucous membrane;
- purulent discharge;
- odor from the mouth.
Treatment
Treatment is carried out according to the following scheme.
At the first stage, the main sign of the disease is removed - reporting. The procedures are also aimed at normalizing the process of removing fluid from the sinuses. Next, efforts are directed towards eliminating the cause. Most are viruses, so a course of antibiotics is recommended.
Administration of medications through a puncture is indicated. This is done at the first stage of treatment. When the resorption stage begins, the patient is prescribed physiotherapy and massage. It is possible to use UHF currents, inhalations, and acupuncture.
To understand that sinusitis has been cured, you can take a repeat x-ray. It will clearly show the dynamics of the disease. If necessary, a second course of treatment is prescribed or the current one is adjusted.
How do you know if sinusitis is going away? Symptoms gradually disappear: temperatures normalize, pus disappears in the discharge, pain disappears, and the general condition of the body improves. However, you should not rejoice ahead of time. It is important to complete treatment even if it seems that everything is over.
Prevention
Sinusitis is a serious ENT disease. Therefore, you definitely need to know how to avoid sinusitis.
You need to start taking measures against this disease already when a runny nose first appears. Under no circumstances should you run it. You need to understand that untreated rhinitis is the greatest risk of further complications. And excuses like “I treated you” won’t help here. After a course of therapy prescribed by a doctor, you need to check the result of the treatment.
You can give a number of tips to prevent the disease:
- avoid hypothermia;
- strengthen your immune system;
- Treat ENT diseases in a timely manner.
conclusions
Sinusitis is a viral disease accompanied by inflammation of the upper sinuses. At first glance, it looks like a regular runny nose. But later painful sensations appear, the temperature rises, and pus appears in the discharge.
In this case, you should immediately go to the hospital. After conducting a series of studies, the doctor will be able to make a correct diagnosis and prescribe effective treatment.
You can understand that sinusitis has gone away by the absence of symptoms of the disease, as well as by taking a repeat x-ray.
Sinusitis. Dangerous runny nose Live Healthy! Nasal polyps Colds, sore throat, sinusitis. How to understand what is wrong with you and when to go to the doctor? Signs of sinusitis, treatment and prevention Elena Malysheva: Breast cancer stages - signs and symptoms.
Breast cancer treatment! Psychoanalysis of diseases (psychosomatics): sinusitis Psychosomatics: Nose. Runny nose.
Keen sense of smell PERIODONTITIS 10 YEARS - initial stage, how to treat, prevention ✚ HEALTHY! How to recognize sinusitis symptoms How to treat and cure fungal sinusitis How to avoid the consequences of sinusitis. About a new effective treatment method
Source:
How many days does sinusitis take to be treated: how long does treatment take?
A definite answer to the question “how long is sinusitis treated” can only be done by making an accurate diagnosis. After all, the duration of treatment directly depends on the form of the process, its stage and the presence of complications. Also, other factors can play an important role, such as the state of the body’s immune system, the adequacy and timeliness of treatment.
Most often, sinusitis develops in adults due to the anatomical features of the paranasal sinuses in children.
The microflora that provokes the disease can be viral or bacterial. Usually the trigger is precisely viruses that provoke the catarrhal form of sinusitis, which almost no one pays due attention to.
After a few days, bacterial agents also join in, and a purulent process develops. Another type that stands somewhat apart from external infectious factors is odontogenic sinusitis, which develops due to problems in the oral cavity.
The allergic form stands somewhat apart, in which the inflammatory process has other causes.
Treatment of odontogenic sinusitis
This process is always bacterial in nature and can occur in catarrhal or purulent form. Typically, the catarrhal form lasts about two days, after which a purulent process begins. Yellow or green pus begins to discharge from the nose, sometimes it has a very unpleasant odor.
This process can be both acute and chronic, with exacerbations usually occurring during the cold season. The height of the period is marked by very vivid symptoms, with adequate treatment of which recovery occurs quite quickly.
Complete recovery does not occur until the lesion in the oral cavity is eliminated.
Very often, odontogenic sinusitis is treated in a hospital, since one of the methods of treating the pathology is sinusotomy. During the operation, the maxillary sinus is cleaned and dental problems are eliminated.
How long the intervention will take depends on various factors, but it usually lasts several hours due to the difficulty of access.
After surgical treatment, antibacterial and anti-inflammatory drugs are prescribed for an average of 7-10 days, after which the sutures are removed and the patient is discharged home.
How to treat chronic sinusitis –
If you have chronic maxillary sinusitis, treatment should also begin with determining the cause and source of infection. Patients who are treated for purulent and polypous sinusitis are usually always severe. These are patients with a long history of self-medication and antibiotic use. Many of them then have to be sent for radical maxillary sinusotomy in a hospital setting, but in some cases more gentle techniques can be used.
Modern methods for diagnosing chronic sinusitis are CT or endoscopic endonasal maxillary sinusoscopy. As for treatment methods, this is still lavage of the sinuses using the YAMIK sinus catheter and antibiotic therapy, which in most cases are supplemented by surgical techniques - such as endoscopic endonasal maxillary sinusotomy or radical maxillary sinusotomy.
Computed tomography (CT) - at the diagnostic stage, it is important to do a CT scan and evaluate the condition of the sinus mucosa, whether there are inflammatory foci at the apexes of the roots of the 5-6-7 upper teeth on this side, how well the root canals in these teeth are sealed. Sometimes it happens that the apices of the roots are located immediately under the mucous membrane of the maxillary sinus. In these cases, infection from poorly filled root canals directly affects the mucous membrane of the sinus, without the formation of a traditional inflammatory focus in the area of the apex of the tooth root.
But in some cases, this can lead to the development of an inflammatory focus in the form of a cyst, which penetrates the maxillary sinus and is filled with pus. As we said above, such cysts can only be diagnosed outside the period of exacerbation (when the sinus is not filled with pus), using CT or endoscopic sinusoscopy.
Endoscopic endonasal maxillary sinusoscopy - in some cases it is important to do a diagnostic endoscopic maxillary sinusoscopy - it is done through the nose using a thin flexible probe with a video camera. This allows you to look at the sinus from the inside (determine the presence of polyps and the degree of damage to the sinus, etc.), and also decide whether it is necessary to expand the anastomosis between the sinus and the nasal cavity. In the price list, this service may also be called “Diagnostic endoscopy of the maxillary sinuses,” and its cost on average will be about 2,000 rubles for 1 sinus.
Carrying out endoscopic maxillary sinusoscopy:
Commentary on the video - in the sinus, the tops of the three roots of the 7th tooth are clearly visible, which are visible through the mucous membrane, as well as a cyst up to 1 cm in size (having a round shape and yellow color), filled with pus. Endoscopic sinusoscopy is performed under local anesthesia.
Surgical treatment methods (sinusrotomy) –
1) Endoscopic endonasal maxillary sinusotomy - based on the results of diagnostic maxillary sinusoscopy (if there are polyps, foreign bodies in the sinus, etc.) - endoscopic gentle maxillary sinusotomy is prescribed using the “shaver” apparatus. This device allows you to scrape out polypous growths from the sinus, preventing the need for a full-fledged maxillary sinusotomy in a hospital setting. During this operation, the anastomosis is also widened, which will improve the outflow from the sinus (this will significantly reduce the risk of new exacerbations of chronic sinusitis). The operation is performed under general anesthesia.
2) Radical maxillary sinus - radical maxillary sinus is indicated when most of the mucous membrane of the maxillary sinus is affected (with irreversible changes). If endoscopic maxillary sinusotomy is done through the nose and is a fairly mild procedure, then radical maxillary sinusotomy requires making an incision in the oral cavity and creating a “window” in the bone tissue in the projection of the roots of the 5-6-7 teeth. Through this window, the irreversibly altered mucous membrane is removed, polyps are scraped out, and foreign bodies (tooth fragments or filling material) are removed.
At the same time, reversible edematous-infiltrative changes in the sinus mucosa are not an indication for its radical removal. Those. in case of chronic catarrhal sinusitis, of course, there is no need to perform a radical maxillary sinusitis. In general, nowadays, with the advent of the possibility of performing endoscopic operations using a shaver, the need for radical maxillary sinusotomy has become significantly lower. But this radical technique is really necessary in difficult situations, for example, when chronic sinusitis is observed against the background of an oroantral communication (fistula between the sinus and the oral cavity).
Diagnostics
The diagnosis of acute sinusitis is established on the basis of data obtained from collecting complaints and anamnesis, conducting an objective examination, as well as a number of additional studies. An important role is played by anterior, middle and posterior rhinoscopy, performed sequentially. In addition, radiography of the paranasal sinuses in two projections, ultrasound, computed tomography or magnetic resonance imaging of the paranasal sinuses are indicated.
Rhinoscopy is the main method for diagnosing sinusitis
A general and biochemical blood test and a general urinalysis are prescribed (nonspecific signs of inflammation are detected). To identify the infectious agent, a microbiological study of the punctate is carried out to determine the sensitivity of the pathogen to antibiotics. Cytological examination of imprints of the mucous membrane of the nasal turbinates makes it possible to determine the signs of an incipient inflammatory process in the early stages of the development of the disease.
Treatment of sinusitis (case study) –
A 28-year-old patient came to the medical center with symptoms of unilateral acute purulent maxillary sinusitis (Fig. 15-16). A CT scan revealed that the sinus was half filled with pus. The treatment that was prescribed was punctures and rinsing of the sinuses with antiseptics and massive antibiotic therapy. As a result, for the next 3 years the patient regularly visited this clinic with symptoms of exacerbation of chronic sinusitis, and she was given the same therapy.
During this time, the attending physician never referred the patient to a dentist to determine how well the root canals in teeth 5-6-7 on this side were filled. Moreover, during this time the patient had CT images taken outside the exacerbation period. When the patient comes to me for a consultation, the image taken outside the exacerbation period shows a rounded formation up to 1 cm in size in the area of the bottom of the maxillary sinus, which is not typical for the topography of the sinus (Fig. 17). The preliminary diagnosis is a cyst of the maxillary sinus on the right (in the picture the right sinus is shown on the left).
Own cysts of the sinus mucosa are extremely rare, and practically the only reason for their formation is inflammation in the area of the apex of the roots of one of the 5-6-7 upper teeth. In addition, the CT scan clearly showed that the apices of the roots are located directly under the mucous membrane of the sinus, i.e. There is no layer of bone between the tips of the roots and the bottom of the sinus. As a result, I refer the patient for a “diagnostic maxillary sinusoscopy,” which involves the use of a thin flexible probe with a video camera and light. As a result, we see a cyst filled with pus (Fig. 18). The cyst was located in the projection of 5-6 teeth and we were unable to accurately determine the causative tooth (including because the root canals of all 5-6-7 teeth on this side were poorly sealed).
As a result, the patient was initially referred for an endoscopic maxillary sinusotomy using a shaver (through the nose), a technique used to curettage and remove polyps and cysts in the sinus. During the operation, the patient also had the anastomosis between the maxillary sinus and the nasal cavity widened. 1 month after the operation and repeated diagnostic maxillary sinusoscopy, the patient was sent for retreatment of 5-6-7 teeth (including sanitation of the root canals using preparations based on calcium hydroxide). As a result, the patient is happy and satisfied.
Important: as an oral and maxillofacial surgeon, I sincerely recommend that (if the ENT doctor himself does not consider it necessary to refer you for a CT scan of your teeth, as well as for a consultation with a dentist), you independently consult a dentist-therapist for a consultation. So that a thorough examination of each root canal in the area of 5-6-7-8 teeth is carried out. Unfortunately, ENT doctors make a lot of mistakes in diagnosing the odontogenic nature of the origin of sinusitis, i.e. when it is related to teeth.
Prevention
Acute sinusitis quickly becomes chronic, causing extremely negative consequences. In its advanced form it is difficult to treat. This disease is easier to prevent, as are its possible complications and consequences. To do this, it is enough to pay attention to your health and take preventive measures, which include:
- Regular exposure to fresh air.
- Constant ventilation of living spaces and wet cleaning.
- Timely treatment of viral and infectious diseases, preventing their transition to a chronic form.
- Elimination of congenital anatomical anomalies, for example, a deviated nasal septum.
- Treatment of dental diseases.
- Protecting the nose and mucous membranes from injury and mechanical damage.
- Quitting bad habits such as smoking and regular consumption of alcoholic beverages.
People who work in hazardous industries and have constant contact with chemicals should not forget about safety precautions, protecting their respiratory organs with special means while working. You need to be careful when swimming in pools and open water, preventing large amounts of water from getting into your nose. If a person is prone to allergic reactions, it is necessary to avoid contact with the irritant if possible and take antihistamines on time to prevent a decrease in the protective forces of the immune system.
Factors predisposing to the development of sinusitis –
We have already said that each maxillary sinus communicates with the nasal passages through a special anastomosis (opening). This hole is necessary for the outflow of mucous secretions accumulating in the sinus, as well as for ventilation of the sinus. Moreover, it should be noted that infection of the maxillary sinuses by pathogenic bacteria of the nasal cavity occurs precisely through these anastomosis (and regularly), but in most people this does not end with the development of sinusitis. And there are reasons for this.
Normally, bacteria that enter the sinuses are removed from the sinuses (along with mucus) through the same anastomosis, which occurs due to the movement of the cilia of the ciliated epithelium - the uppermost layer of the mucous membrane of the sinuses. Thanks to this cleansing mechanism, the number of pathogenic bacteria is almost always below a critical level, which would necessarily lead to the development of sinusitis. But in some cases, there is a disruption in the evacuation of mucus and bacteria from the sinuses. And let's look at what this is connected with
Sharp swelling of the nasal mucosa due to influenza, ARVI, chronic rhinitis leads to narrowing or complete closure of the anastomosis between the maxillary sinus and the nasal cavity. As a result, mucus and bacteria accumulate in the sinus lumen, and sinus ventilation (aeration) is also disrupted, which very quickly leads to rapid growth of bacteria. In some patients, these anastomosis may initially be too small in size, which, if even slight swelling occurs, immediately leads to disruption of the outflow of secretions from the sinus. And this is the first moment predisposing to the development of sinusitis.
In such patients, ENT doctors can expand the size of the anastomosis, which will significantly reduce the risk of developing sinusitis in the future. The second predisposing point is the insufficiency of the function of the ciliated epithelium, which provides drainage function, clearing the sinus of mucus. All kinds of chronic rhinitis (including allergic), accompanied by prolonged swelling of the mucous membrane, often lead to disruption of the functioning of the cilia of the ciliated epithelium. Well, the third factor predisposing to the development of sinusitis is when there is a combined infection, i.e. both from the side of the nose and from the tops of the roots of the 5-6-7 upper teeth.
Answers to popular questions
- Is it possible to warm your nose if you have sinusitis? If you have sinusitis, you should not warm your nose. This is a direct contraindication during the acute stage of the inflammatory process. Warming up can not only relieve a person from the disease, but can also lead to a worsening of the patient’s condition, with the spread of infection into the deep structures of the skull.
- Can you do inhalations for sinusitis? Inhalations for sinusitis can be done if this method of treatment was recommended by an otolaryngologist after examining the patient.
- Is it possible to go to the bathhouse if you have sinusitis? Going to the bathhouse is contraindicated in case of acute sinusitis, as there is a risk of the contents of the nasal sinus breaking into the bloodstream. In addition, the bath is prohibited against the background of high body temperature, which almost always accompanies the development of sinusitis.
Complications of maxillary sinusitis –
Acute purulent sinusitis of the maxillary sinus (or with exacerbation of chronic sinusitis) can be complicated by the development of purulent periostitis of the upper jaw, the formation of an abscess or phlegmon of the orbit, as well as the transition of inflammation to other nasal sinuses, including the cells of the ethmoid labyrinth. In addition to these complications, phlebitis and thrombophlebitis of the veins of the face, as well as the sinuses of the dura mater, can occur, which, along with phlegmon of the orbit, can even lead to death.
As for long-term chronic forms of sinusitis (purulent and polypous forms), the prognosis for them is favorable only with surgical treatment, i.e. when performing endoscopic maxillary sinusotomy using a shaver or radical maxillary sinusotomy in a hospital setting. Long-term chronic sinusitis also leads to impaired immunological reactivity and immune deficiency.
Sources:
1. Higher medical education of the author, 2. Based on personal experience in maxillofacial surgery, 3. “Guide to maxillofacial surgery” (Timofeev A.A.), 4. “Complex treatment of odontogenic maxillary sinusitis” (Shulman F. ), 5. “Clinical recommendations for the diagnosis and treatment of acute rhinosinusitis” (Lopatin A.S., Svistushkin V.M.).
Possible complications and consequences
Possible complications of sinusitis in adults are:
- Penetration of infection and pus into the brain with the development of meningitis and meningoencephalitis. The disease is manifested by headache, nausea, vomiting and impaired consciousness.
- Eye damage (conjunctivitis, keratitis, retrobulbar abscess formation, exophthalmos, optic nerve damage, blindness).
- Anosmia (loss of the ability to distinguish odors).
- Frequent inflammatory diseases of the oral cavity. The reason is breathing through the mouth.
- Otitis.
- Purulent sore throat.
- Osteomyelitis of bones.
- Sepsis.
- Pyelonephritis (infectious inflammation of the kidneys). Develops when bacteria spread through the blood.
- Myocarditis.
- Complications during pregnancy.
- Empyema.
- Destruction of the bones adjacent to the sinuses.
- Thrombosis of the venous sinuses.
- Spread of the pathological process to adjacent sinuses.
Pathogenesis of chronic sinusitis
The formation of the paranasal sinuses in a child occurs when he is still in the womb. From birth until 20 years of a person’s life, they gradually “mature.” Thus, in infants there are no frontal sinuses, while the remaining sinuses are in their infancy and gradually form as the child grows and the bones of his face increase.
Goblet cells of the ciliated epithelium, covering the sinuses from the inside, take part in the formation of mucus. Mucus moves to the anastomosis (openings) of the paranasal sinuses due to the movement of the cilia of the epithelium. Typically the speed of such advancement is 1 cm/min. The size and diameter of the anastomosis are small and equal to approximately 1-2 mm.
Symptoms of hypertrophic rhinitis
The main manifestations of hyperplastic rhinitis include difficulty in nasal breathing and constant nasal congestion. Patients complain of mucous and purulent discharge from the nose, mainly in the morning. Over time, vasoconstrictor and anti-inflammatory therapy loses its effectiveness. Breathing is primarily through the mouth, which causes dry mouth, snoring, and episodes of sleep apnea. Subsequently, a sensation of a foreign body in the nasopharynx, increased fatigue, aching headache, and insomnia occur. The ability to perceive odors decreases, leading to loss of smell (anosmia). Patients experience a change in voice timbre (closed nasality). Self-cleansing of the nasal passages from pathological secretions causes damage to the mucous membrane, as a result, increased bleeding.
Treatment of hypertrophic rhinitis
Conservative therapy is effective only in the initial stages of the disease. During this period, vasoconstrictor and anti-inflammatory drops are used, ultraviolet irradiation of the nasal cavity, exposure to high-frequency radiation, and nasal massage using 20% splenin ointment are prescribed. In case of diffuse proliferation of tissues of the mucous layer of the nasal cavity and the ineffectiveness of conservative therapy, the only treatment method is surgery. Surgical intervention is a mechanical, laser, thermal effect on the affected part of the nasal concha in order to restore nasal breathing, sense of smell and prevent further pathological growth of the mucous membrane. The following types of operations are performed:
- Conchotomy (submucosal, total, partial) – excision of a section of the mucous layer of the lower and middle parts of the nasal concha. If the periosteum and bone tissue are involved in the pathological process, partial or complete removal of the inner lining of the nasal cavity along with bone elements is performed (osteoconchotomy).
- Cryodestruction is the effect on hypertrophied areas with a special applicator cooled with liquid nitrogen.
- Laser vasotomy – coagulation of vessels located under the mucous layer of the nasal cavity. Used for mild illness.
- Ultrasonic disintegration of the nasal passages - sclerosis of the blood vessels of the nasal cavity under the influence of ultrasound.
Hypertrophic rhinitis
Hypertrophic rhinitis
is an inflammatory disease of the nasal cavity, which is characterized by the proliferation of the mucous membrane lining it. In advanced cases, inflammation involves bone elements and periosteum. The main symptoms are nasal congestion, difficulty breathing, nasal tone, and occasional headache. Diagnosis of rhinitis includes examination by an otolaryngologist with rhinoscopy and endoscopy. To clarify the diagnosis, X-rays and CT scans of the paranasal sinuses are performed. Treatment at the initial stage is conservative, with the prescription of anti-inflammatory, vasoconstrictor drops. In case of diffuse damage, surgery is performed to remove pathological growths of the mucous layer or bone tissue.