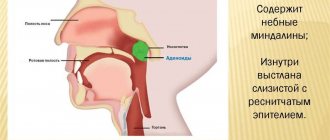
Follicular tonsillitis is the most common form of inflammation of the lymphoid ring in the throat. The disease is accompanied by enlargement and inflammation of the cervical regional lymph nodes, into which lymph flows from foci of inflammation. The main risk group for the development of this pathology are children and young people, while follicular tonsillitis in adults after forty years of age is classified as a rare disease.
In adults, this disease occurs as an exacerbation of chronic tonsillitis, or as a result of complications of catarrhal processes. Lack of help for this disease leads to the development of many complications, so it is very important to know how to treat follicular tonsillitis correctly at home.
What it is
This is a bacterial inflammation of the tonsils, which is accompanied by the accumulation of pus in the follicles (lymphoid tissue) of the organ. A visual examination reveals the appearance of white-gray lesions on the surface of the tonsils. These purulent plugs appear against the background of general intoxication of the body, increased body temperature and sore throat on days 1-3 of the disease.
In the International Classification of Diseases (ICD 10), follicular tonsillitis with streptococcal etiology has the code - J03.0, for other pathogens (mainly staphylococci) - J03.8. Also, if the patient experiences 2 or more episodes per year, then a diagnosis of chronic tonsillitis is made, which requires a slightly different approach to treatment.
Pathogenesis
- Group A beta-hemolytic streptococcus infects epithelial cells located on lymphoid tissues.
- Lipoteichoic acid associated with M-protein ensures reliable fixation and penetration of the pathogen into the cell.
- M-protein inhibits the phagocytic abilities of macrophages in relation to the pathogen.
- The microorganism causes cell death by purulent melting. The process involves not only epithelial cells, but also the parenchyma of the tonsils.
In the natural anatomical structures of the tonsils - the follicles - a necrotic mass accumulates, which is visible only macroscopically.
Symptoms
Clinical signs of follicular sore throat are usually divided into general and local. The bacteria that cause acute tonsillitis produce a huge amount of toxins, which leads to the development of the following symptoms:
increase in body temperature to high levels (up to 39.5°C);
aching or squeezing headaches;
severe general weakness, reduced performance;
disorders of the functioning of the digestive system (lack of appetite, nausea, vomiting, feeling of heaviness in the stomach);
muscle and joint pain;
During a local examination of the oropharynx, the following symptoms attract attention:
redness of the mucous membrane of the posterior wall of the oropharynx;
an increase in the size of the palatine tonsils, their pronounced swelling;
the appearance of “purulent plugs” on the surface of the tonsils in the form of separate foci;
when you press the tonsils with a spatula, a small amount of purulent exudate is sometimes released;
dryness of the oral mucosa.
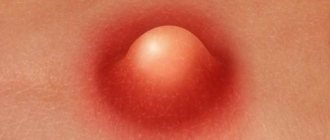
Diagnosing follicular tonsillitis in children is quite simple with a simple visual examination of the patient’s oropharynx. You can see an example of what follicular tonsillitis looks like in the photo below.
Prevention
You can get rid of follicular tonsillitis only by following all medical prescriptions. But how to avoid relapse of the disease? A necessary condition for strengthening the immune system is proper nutrition and adherence to the drinking regime. Spicy foods, carbonated drinks, strong tea and coffee, chips and salty crackers irritate the mucous membrane, so it is better to avoid such products. Regular consumption of dairy products, eggs, vegetables and fruit juices, and whole grain cereals will help improve your well-being.
Recommendations to drink cold water can only do harm, because it is not the throat that needs to be hardened, but the body as a whole. This is not an easy process that requires an integrated approach and patience. The beginning of hardening is taking a cool shower, long walks in cool weather or aerotherapy, sunbathing - heliotherapy during safe hours (from 8.00 to 11.00 and after 16.00), walking barefoot. All methods of strengthening the body must be combined with regular physical exercise to lift your mood, feel a surge of strength and vigor.
Additionally, natural immunostimulants will strengthen the body: ginseng, eleutherococcus.
Following nutritional recommendations and performing healing procedures will allow you to forget about tonsillitis forever.
Treatment
Therapy must be comprehensive. It includes both the use of specific antibacterial drugs and symptomatic treatment. It usually takes place on an outpatient basis, but it is better to hospitalize children or patients with concomitant somatic pathologies in the otolaryngology or infectious diseases department of the hospital. Antibiotics are key.
Antibacterial therapy
Amoxicillin with clavulanic acid
To cure follicular tonsillitis, protected penicillins are first prescribed. Among them, the most commonly used combination is amoxicillin with clavulanic acid. The presence of the latter component makes it possible to overcome the resistance of some microorganisms that produce beta-lactamase enzymes that are capable of breaking down the antibiotic. It can be prescribed to patients of any age, starting from the first year of life (in syrup form).
This antibiotic has a bactericidal effect against most strains of bacteria that cause tonsillitis. Its molecules are capable of destroying the integrity of the cell membranes of pathogenic microorganisms. At the same time, the drug has a good bioavailability (absorption in the digestive tract).
The only significant contraindication to the use of a combination of amoxicillin with clavulanic acid is the presence of hypersensitivity in the patient to penicillin antibiotics. The drug is prescribed with caution for chronic kidney diseases.
The following side effects are possible when using this medication:
allergic reactions (appearance of a red rash on the skin with severe itching, indigestion, swelling, anaphylactic shock with hemodynamic disturbances);
functional disorders of the stomach and intestines (symptoms of nausea, vomiting, diarrhea, feeling of heaviness in the abdomen or aching pain);
temporary increase in the concentration of liver enzymes;
the addition of a secondary bacterial or fungal infection;
decrease in the number of blood cells in the general analysis.
For the treatment of purulent sore throat in adults or children weighing over 40 kg, the drug is prescribed in the form of tablets at a dosage of 875/125 mg 2 or 3 times a day. For the treatment of children, there are tablets of 500/125 mg or 250/125 mg, as well as syrup. The latter is especially convenient for use for a child in the first two years of life, since it allows you to select an individual dose based on age and body weight. The duration of therapy is usually from 5 to 14 days.
Azithromycin
The effectiveness of therapy for follicular angina is assessed after 48-72 hours. If after this period of time there is no positive dynamics during treatment with penicillin antibiotics, then the drug is changed to a macrolide (azithromycin or clarithromycin).
The advantage of azithromycin is that it is able to accumulate in the respiratory epithelium of the airways and maintain a therapeutic concentration for about 3 days after the last dose, which is very convenient for the patient. Its mechanism of action is bacteriostatic - antibacterial molecules block protein synthesis in microbial cells, which makes further protein synthesis and reproduction impossible. Indicators of microflora resistance to macrolides remain at low levels.
The use of azithromycin is not recommended in the presence of hypersensitivity to macrolides, severe heart failure, or end-stage renal impairment. When prescribed for myasthenia gravis, a decrease in the effectiveness of specific therapy for this disease was observed.
It is necessary to highlight the following undesirable effects when using an antibiotic:
functional digestive disorders;
attachment of fungal microflora on the skin or mucous membranes (mainly the oral cavity);
temporary impairment of vision;
tachycardia in patients with congenital anomalies of the cardiac conduction system;
inhibition of the hematopoietic system with manifestations of anemia, decreased immunity and hemorrhages;
toxic liver damage;
sleep disturbances (drowsiness or difficulty falling asleep).
The usual azithromycin treatment regimen for an adult patient consists of taking one 500 mg tablet of the drug per day, regardless of food. There is syrup for children, and the daily dose is calculated based on the ratio of 10 mg per 1 kg of body weight per day. The duration of antibiotic therapy is from 3 to 10 days.
Epidemiology
The source of infection is a patient or a carrier of group A beta-hemolytic streptococcus. These can be adults or children who carry:
- tonsillitis;
- sore throat;
- scarlet fever;
- streptoderma and other pathological conditions caused by this pathogen.
There are airborne or aerogenic, food and contact-household routes of transmission of infection. Beta-hemolytic streptococcus selectively affects reticuloendothelial tissue:
- tonsils;
- The lymph nodes;
- adenoids and so on.
Important! Follicular tonsillitis most often affects children aged 3 to 7 years, when there is frequent contact with the bacterium (it is at this age that the child begins to attend children's groups), adults get sick much less often.
The occurrence of the disease in children of the first year of life is casuistry due to the action of antimicrobial and antitoxic immunity received from the mother, as well as due to the anatomical and physiological features of the structure - poor differentiation of the Pirogov lymphoid ring.
Also, older people are less susceptible to this disease due to age-related hypoplasia of lymphoid tissue in this population group.
The peak incidence occurs in the autumn-winter period, when the frequency of exacerbation of chronic tonsillitis and the occurrence of respiratory infections increases, and the protective properties of the immune system decrease.
Complications
Complications of follicular tonsillitis are usually divided into early and late. Early ones are caused by the active development of the primary bacterial focus and the weak response of the patient’s immune system. They usually develop in the first days of the disease. They are also facilitated by inadequate therapy and refusal to use antibiotics with obvious signs of bacterial tonsillitis. Early complications of follicular tonsillitis include:
generalization of the infectious process with the development of sepsis;
necrotic process in the tonsils;
bacterial inflammation of the middle ear (acute otitis media) or paranasal sinuses (sinusitis).
Late complications of follicular tonsillitis have an autoimmune mechanism of development. Some antigens that are on the surface of streptococci are almost identical to the proteins of the body's own tissues. And the body sometimes ceases to distinguish between them, producing antibodies that cause inflammatory processes in various organs. These complications include:
acute rheumatic fever with damage to the heart and joints;
acute glomerulonephritis (damage to the glomerular system of the kidneys).
Source
Causes
The main cause of sore throat is contact with the source of infection (that is, the patient). As already noted, the disease has a very high spread, so the risk of getting sick after contact is very high. Another possible reason is a malfunction in the body (other infections, hypothermia, etc.), as a result of which immunity is reduced and microorganisms present in the throat are activated. As a conclusion, you should avoid contact with people with tonsillitis, and increase the body’s defenses in every possible way.
general information
Short description
Acute tonsillitis is a common acute infectious-allergic disease with local manifestations in the form of acute inflammation of one or more components of the lymphadenoid pharyngeal ring, most often the palatine tonsils.
Chronic tonsillitis is a persistent chronic inflammation of the tonsils with a general infectious-allergic reaction.
Correlation of ICD-10 and ICD-9 codes
| ICD-10 | ICD-9 | ||
| Code | Name | Code | Name |
| J03 | Acute tonsillitis | 28.19 | Other diagnostic manipulations on the tonsils and adenoids |
| J03.0 | Streptococcal tonsillitis | 28.20 | Tonsillectomy without adenoid removal |
| J03.8 | Acute tonsillitis caused by other specified pathogens | 28.30 | Tonsillectomy with adenoid removal |
| J03.9 | Acute tonsillitis, unspecified | 28.60 | Removal of adenoids without tonsillectomy |
| J35.0 | Chronic tonsillitis | 28.70 | Stopping bleeding after tonsillectomy and adenoid removal |
| 28.99 | Other manipulations on the tonsils and adenoids | ||
| 29.19 | Other diagnostic manipulations on the pharynx | ||
Protocol development date: 2021.
Users of the protocol : general practitioners, otorhinolaryngologists, infectious disease specialists, hematologists.
Patient category: adults.
Level of evidence scale:
| A | A high-quality meta-analysis, systematic review of RCTs, or large RCTs with a very low probability (++) of bias, the results of which can be generalized to an appropriate population. |
| IN | High-quality (++) systematic review of cohort or case-control studies, or High-quality (++) cohort or case-control studies with very low risk of bias, or RCTs with low (+) risk of bias, the results of which can be generalized to an appropriate population . |
| WITH | Cohort or case-control study or controlled trial without randomization with low risk of bias (+). The results of which can be generalized to the relevant population or RCTs with very low or low risk of bias (++ or +), the results of which cannot be directly generalized to the relevant population. |
| D | Case series or uncontrolled study or expert opinion. |
Provoking factors, risk group
People with diseases of the immune system and children are more susceptible to infection than other categories of citizens.
Dust and gas pollution in large cities increases the load on the respiratory system, increasing the likelihood of illness.
The risk group also includes people working in enterprises with increased hazards.
Some factors that reduce immunity and provoke the development of infection in the respiratory system include:
- Hypothermia.
- Smoking.
- Long-term use of hormonal drugs.
- Untreated small foci of infection (caries, gum inflammation).
- Mechanical throat injuries.
- The recovery period after illnesses and operations.
- Lack of vitamins.
- Unbalanced diet.
- Severe stressful situations.
- Metabolic disease.
Read more about the causes of infection with follicular tonsillitis in our video:
https://youtube.com/watch?v=ZgqjCEvULJg
Classification
Classification (according to I.B. Soldatov) [1]
I. Acute tonsillitis:
Primary tonsillitis: · catarrhal; lacunar; · follicular; · ulcerative-membranous.
Secondary tonsillitis: · in acute infectious diseases - diphtheria, scarlet fever, measles, tularemia, typhoid fever; · for diseases of the blood system - infectious mononucleosis, agranulocytosis, alimentary-toxic aleukia, leukemia.
II. Chronic tonsillitis:
Nonspecific: · compensated form; · decompensated form.
Specific: · for infectious granulomas, tuberculosis, scleroma, syphilis, scleroma.
In adults
Although an adult’s body is much stronger than a child’s, and the immune system is stronger, it is not even easy for him to endure a sore throat. Especially if there is a delay in contacting a specialist or inadequate treatment.
Sore throat during breastfeeding is also more than unpleasant, when the antibiotics necessary for treatment can pass through the mother’s milk to the baby and harm him. That is why pregnant and breastfeeding women should be even more careful, and if necessary, immediately consult a doctor, who is obliged to make the most appropriate decisions according to the situation.
Diagnostics (outpatient clinic)
OUTPATIENT DIAGNOSTICS**
Diagnostic criteria
Complaints: sore throat, weakness, headache, fever, chills, loss of appetite.
Catarrhal sore throat: burning sensation, dryness, sore throat, moderate sore throat, aggravated by swallowing, low-grade body temperature, malaise, weakness, headache.
Follicular sore throat: severe sore throat, sharply increasing when swallowing, with irradiation to the ear, increased body temperature to 38-40 ° C, difficulty swallowing, symptoms of intoxication - headache, weakness, chills, sometimes pain in the lower back and joints.
Lacunar tonsillitis: the same as follicular tonsillitis, but it is more severe.
Complaints: frequent sore throats, low-grade fever, pain in muscles, joints, weakness, lethargy, fatigue, sleep disturbance.
History: previous tonsillitis, especially without antibiotic treatment, impaired nasal breathing.
Physical examination:
Acute tonsillitis: with pharyngoscopy:
Catarrhal tonsillitis: diffuse hyperemia and swelling of the palatine tonsils.
Follicular tonsillitis: diffuse hyperemia, infiltration and swelling of the tonsils, the presence of yellowish-white purulent spots on the surface of the tonsils.
Lacunar tonsillitis: hyperemia and swelling of the palatine tonsils, the surface of the tonsils is covered with purulent plaque of various shapes.
On palpation: enlargement and tenderness of regional lymph nodes.
Chronic tonsillitis: with pharyngoscopy: liquid pus or caseous-purulent plugs in the lacunae (may have an odor); · Giese sign – congestive hyperemia of the edges of the palatine arches; Zach's sign - swelling of the upper edges of the anterior palatine arches; · Preobrazhensky’s sign – roller-like thickening of the edges of the anterior palatine arches; · fusion and adhesions of tonsils with arches and triangular fold; · tonsils are small with a smooth or loose surface; · enlargement of individual regional lymph nodes, sometimes painful. On palpation: in the absence of other foci of infection in this region.
Laboratory tests: · UAC; · OAM; · throat swab BL.
Instrumental studies: · pharyngoscopy; · ECG.
Diagnostic algorithm: (diagram)
Proper care for a sick child
If the disease is diagnosed in a mild form, the child can be treated on an outpatient basis.
In this case, you must adhere to the following rules and recommendations:
- Avoid any contact with peers and maintain bed rest.
- You can go outside and bathe your child only if the temperature has returned to normal (36.6 degrees).
- Follow a regimen of increased consumption of warm liquids (rosehip decoction, tea with lemon and honey, hot raspberry or currant compote).
- Food should be neutral, and if possible pureed. It is prohibited to include spicy, salty and sour foods in the menu.
- Maintain proper ventilation of the room and carry out wet cleaning.
- Cutlery and hygiene items must be strictly individual.
- Be sure to follow all the recommendations prescribed by the doctor.
Diagnostics (hospital)
DIAGNOSTICS AT THE INPATIENT LEVEL**
Diagnostic criteria at the inpatient level**: see outpatient level.
Diagnostic algorithm: see outpatient level.
List of main diagnostic measures:
— for acute tonsillitis: · OAC; · OAM; · feces on worm eggs; · blood on RW; · smear on BL.
— for chronic tonsillitis: · histological examination of surgical material (palatine tonsils).
List of additional diagnostic measures: no.
Folk remedies
- For gargling:
- Lemon acid.
- Elderberry decoction.
- Beetroot juice with the addition of vinegar (no more than 15 ml of vinegar per glass of juice).
- Salt.
- Carrot juice.
- Pharmaceutical camomile.
- Eucalyptus herb infused for 20 minutes in hot water.
- Add beaten egg white and a teaspoon of salt to a glass of warm water. The components are mixed until the mixture is homogeneous.
- Teas:
- Linden with honey.
- Cranberry.
- With thyme.
- With rose hips.
- Raspberry, sage, and St. John's wort leaves also have an anti-inflammatory effect.4. For sore throat, people often inhale pine buds or chew a piece of dried pine resin in the mouth without swallowing.
Features of treatment during pregnancy
Pregnant women with follicular tonsillitis are required to undergo a course of antibiotics. This poses less risk to the development of the fetus than no appropriate treatment. Basically, preference is given to aerosol topical antibiotics and modern drugs approved for pregnant women.
The high temperature of the expectant mother can cause congenital defects in the baby, so before the doctor arrives, you must try to reduce it. Wiping your feet with a vinegar-alcohol solution and a paracetamol tablet will help in most cases.
- You should not take aspirin, it reduces blood clotting, increasing the risk of bleeding.
- Thermal procedures are also extremely undesirable. They can cause uterine contractions and premature birth.
- It is better to eat food in small portions in crushed form, but you cannot refuse food.
- Regular gargling will help you cope with the infection faster, but you should be careful when choosing medicinal herbs for this purpose. During pregnancy, the likelihood of allergies to certain natural components increases.
- Stressful situations, especially against the background of illness, are unacceptable.
Physiotherapy
After the acute symptoms of the disease disappear, the doctor may refer the patient for further physiotherapeutic treatment
This is especially important for chronic tonsillitis and in childhood. The following procedures are most commonly practiced:
- Warming up.
- Laser treatment.
- Electrophoresis.
- Phototherapy.
- Magnetotherapy.
- Ultraviolet irradiation of the tonsils.
Resort and sanatorium prevention of relapses is desirable, but during the period of remission it is enough to change the environmental situation to a more favorable one.
Differential diagnosis
For acute tonsillitis
| Diagnosis | Rationale for differential diagnosis | Surveys | Diagnosis exclusion criteria |
| Acute and chronic pharyngitis | A similar clinical picture is a sore throat | Pharyngoscopy | Tonsils are intact |
| Diphtheria of the pharynx | A similar clinical picture - sore throat, plaque on the tonsils, symptoms of intoxication | Pharyngoscopy, throat swab for BL, consultation with an infectious disease specialist | Presence of epidemiological history Diphtheria bacillus culture |
| Scarlet fever | A similar clinical picture - sore throat, plaque on the tonsils, symptoms of intoxication | Pharyngoscopy, consultation with an infectious disease specialist | Presence of epidemiological medical history Presence of pinpoint rash in the lower abdomen, buttocks, groin and inner surface of the extremities |
| Measles | A similar clinical picture - sore throat, plaque on the tonsils, symptoms of intoxication | Pharyngoscopy, consultation with an infectious disease specialist | Presence of Filatov's spots and measles rash |
| Infectious mononucleosis | A similar clinical picture - sore throat, plaque on the tonsils, symptoms of intoxication | Pharyngoscopy, consultation with an infectious disease specialist | The presence of enlarged lymph nodes, in the BC - monocytosis up to 70-90% |
| Leukemia | A similar clinical picture - sore throat, plaque on the tonsils, symptoms of intoxication | Pharyngoscopy, consultation with a hematologist | In the CBC - the presence of blast cells |
| Agranulocytosis | A similar clinical picture - sore throat, plaque on the tonsils, symptoms of intoxication | Pharyngoscopy, consultation with a hematologist | In the UAC – a decrease in the number of leukocytes with the disappearance of granulocytes |
For chronic tonsillitis
| Diagnosis | Rationale for differential diagnosis | Surveys | Diagnosis exclusion criteria |
| Hypertrophy of the palatine tonsils | A similar clinical picture is enlargement of the palatine tonsils | Pharyngoscopy | Absence of local signs of chronic tonsillitis |
| Neoplasm of the palatine tonsils | A similar clinical picture - enlarged palatine tonsils, symptoms of intoxication | Pharyngoscopy, oncologist consultation, histological examination | Absence of local signs of chronic tonsillitis, verification of diagnosis |
| Pharyngomycosis | A similar clinical picture is plaque on the tonsils | Pharyngoscopy, mycological examination | Sowing the fungus |
Consult an experienced specialist without leaving your home!
Health consultation from 2500 tenge / 430 rubles
Interpretation of analysis and research results
Second opinion regarding diagnosis, treatment
Choose a doctor
During pregnancy
During pregnancy, this form is very dangerous. Often the disease even leads to the death of the fetus. The circulation of toxins in the blood, an increase in temperature to exorbitant levels, weakened immunity - all this provokes a miscarriage. If a pregnant woman has signs of a purulent form of sore throat, she should be hospitalized immediately and thoroughly examined.
The doctor must choose medications for treatment in order to select only those that will not harm the unborn child. Thus, most antibiotics are contraindicated for pregnant women, especially in the early stages.
Diet restrictions and bed rest are strictly observed. As basic treatment options, rinses with Furacilin, decoctions, and salt solutions are used. High fever is brought down with Paracetamol. Other antipyretics cannot be used. Fever is extremely dangerous because it can lead to birth defects in the child.
Despite the reluctance to eat during an exacerbation of the disease, pregnant women should not refuse nutrition, since the body especially at this time needs protein foods and vitamins. You should also drink plenty of water, excluding hot and sour drinks.
Self-medication during pregnancy is strictly contraindicated!
Treatment
Drugs (active ingredients) used in treatment
| Azithromycin |
| Amoxicillin |
| Ampicillin |
| Acetylsalicylic acid |
| Benzylpenicillin |
| Josamycin |
| Ibuprofen |
| Nitrofural |
| Paracetamol |
| Povidone - iodine |
| Chlorhexidine |
| Cefazolin |
| Cefuroxime |
Consequences of untreated sore throat
Sore throat must be treated. If parents are negligent about the fact that their child has become infected with this disease, the baby may subsequently experience the following complications:
- inflammatory damage to the lymph nodes, purulent lymphadenitis;
- phlegmon of the neck;
- myocarditis;
- polyarthritis (infectious form);
- rheumatism;
- meningitis;
- sepsis;
- pyelonephritis.
After treatment, the patient must undergo laboratory tests and, if necessary, have an ultrasound of the heart and an ECG. This is necessary so that the pediatrician can make sure that there are no complications.
Treatment (inpatient)
INPATIENT TREATMENT**
Treatment tactics**: see outpatient level.
Surgical intervention
Bilateral tonsillectomy: Indications for 2-sided tonsillectomy: · ineffectiveness of conservative treatment with chemotherapy; · decompensated form of chemotherapy; Chronic chemotherapy complicated by paratonsillitis or paratonsillar abscess; · tonsillogenic sepsis.
Other types of treatment: · wave therapy; · ultrasound therapy; · UHF to regional lymph nodes; · Ural Federal District; · aerosols; · laser therapy; · helium-neon laser radiation; · washing the tonsils according to N.V. Belogolovy.
Indications for specialist consultation: · consultation with specialists in the presence of concomitant pathology.
Indications for transfer to the intensive care unit: · presence of complications after tonsillectomy (bleeding).
Indicators of treatment effectiveness: · after 2-sided tonsillectomy: no complaints of recurrent tonsillitis.
What compresses are not prohibited?
Not all compresses are contraindicated for sore throat in a child. So, doctors allow those that do not warm a sore throat too much, for example, from:
- Cabbage leaves, which are good for relieving inflammation. You need to apply several leaves to the throat, wrap them with cellophane and a scarf on top. Leave overnight.
- Boiled potatoes. You need to crush it and wait until it becomes warm. Then apply it not to the throat, but to the neck. Cover the top with gauze and secure with cling film. Keep until cool.
- Cottage cheese. You need to put about 400-500 grams of cottage cheese at room temperature on cling film, put it on your neck, and wrap it with a cloth. Remove when the curd is completely dry. It is advisable to leave this compress overnight.
Information
Sources and literature
- Minutes of meetings of the Joint Commission on the Quality of Medical Services of the Ministry of Health of the Republic of Kazakhstan, 2021 1) Soldatov I.B.
 Lectures on otorhinolaryngology. - M.: Medicine.-1994.-288p. 2) Soldatov I.B. Guide to otorhinolaryngology. - M.: Medicine. - 1997. - 608 p. 3) Palchun V.T. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2014.-654s. 4) Pluzhnikov M.S., Lavrenova G.V., et al. Chronic tonsillitis. — SPb.-20Yu.-224s. 5) Palchun V.T., Magomedov M.M., Luchikhin L.A. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2008.-649s. 6) National Scientific Center for Expertise of Medicines and Medical Products. https://www.dari.kz/category/search_prep 7) Kazakhstan national form. www.knf.kz British National Formulary.www.bnf.com 9) Edited by prof. L.E. Ziganshina “Big Directory of Medicines.” Moscow. GEOTAR-Media. 2011. 10) Cochrane Library, www.cochrane.com 11) WHO List of Essential Medicines. https://www.who.int/features/2015/essential_medicines_list/com
Lectures on otorhinolaryngology. - M.: Medicine.-1994.-288p. 2) Soldatov I.B. Guide to otorhinolaryngology. - M.: Medicine. - 1997. - 608 p. 3) Palchun V.T. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2014.-654s. 4) Pluzhnikov M.S., Lavrenova G.V., et al. Chronic tonsillitis. — SPb.-20Yu.-224s. 5) Palchun V.T., Magomedov M.M., Luchikhin L.A. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2008.-649s. 6) National Scientific Center for Expertise of Medicines and Medical Products. https://www.dari.kz/category/search_prep 7) Kazakhstan national form. www.knf.kz British National Formulary.www.bnf.com 9) Edited by prof. L.E. Ziganshina “Big Directory of Medicines.” Moscow. GEOTAR-Media. 2011. 10) Cochrane Library, www.cochrane.com 11) WHO List of Essential Medicines. https://www.who.int/features/2015/essential_medicines_list/com
 Lectures on otorhinolaryngology. - M.: Medicine.-1994.-288p. 2) Soldatov I.B. Guide to otorhinolaryngology. - M.: Medicine. - 1997. - 608 p. 3) Palchun V.T. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2014.-654s. 4) Pluzhnikov M.S., Lavrenova G.V., et al. Chronic tonsillitis. — SPb.-20Yu.-224s. 5) Palchun V.T., Magomedov M.M., Luchikhin L.A. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2008.-649s. 6) National Scientific Center for Expertise of Medicines and Medical Products. https://www.dari.kz/category/search_prep 7) Kazakhstan national form. www.knf.kz British National Formulary.www.bnf.com 9) Edited by prof. L.E. Ziganshina “Big Directory of Medicines.” Moscow. GEOTAR-Media. 2011. 10) Cochrane Library, www.cochrane.com 11) WHO List of Essential Medicines. https://www.who.int/features/2015/essential_medicines_list/com
Lectures on otorhinolaryngology. - M.: Medicine.-1994.-288p. 2) Soldatov I.B. Guide to otorhinolaryngology. - M.: Medicine. - 1997. - 608 p. 3) Palchun V.T. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2014.-654s. 4) Pluzhnikov M.S., Lavrenova G.V., et al. Chronic tonsillitis. — SPb.-20Yu.-224s. 5) Palchun V.T., Magomedov M.M., Luchikhin L.A. Otorhinolaryngology. –Moscow “GEOTAR-Media”. -2008.-649s. 6) National Scientific Center for Expertise of Medicines and Medical Products. https://www.dari.kz/category/search_prep 7) Kazakhstan national form. www.knf.kz British National Formulary.www.bnf.com 9) Edited by prof. L.E. Ziganshina “Big Directory of Medicines.” Moscow. GEOTAR-Media. 2011. 10) Cochrane Library, www.cochrane.com 11) WHO List of Essential Medicines. https://www.who.int/features/2015/essential_medicines_list/com