Pneumothorax of the lung is a very dangerous pathology that requires emergency measures to save a person. This phenomenon is generated by the accumulation of air where there should not be any, which disrupts the functions of various organs and causes severe respiratory failure. Incorrect treatment can lead to dire consequences.
An unexpected pneumothorax of the lung can have a catastrophic continuation if the people around you do not get involved in helping. Knowledge of the basics of this pathology can save a human life, since no one is immune from this disease. Pneumothorax can occur in anyone at any age.
Description
Pneumothorax is a pathological condition in which air accumulates in the pleural cavity. Has code J93 according to the ICD. Occurs with injuries and certain diseases of the chest organs. It causes an increase in intrathoracic pressure, causes partial or complete collapse of the lung, and displacement of the mediastinal organs. The rapid accumulation of a significant volume of air poses a danger to the patient's life due to the development of acute respiratory failure, compression of large vessels and cardiac dysfunction.
Reasons for development
There are two main groups of causes of pneumothorax: mechanical and non-mechanical. Mechanical ones include:
- Closed injuries : rib fractures with displacement of fragments, disruption of the integrity of the pleura and lung with bone fragments.
- Open injuries : punctures, stab wounds, less often lacerations and gunshot penetrating wounds of the chest.
- Iatrogenic injuries : lung injuries during medical procedures, for example, placement of a subclavian catheter, pleural puncture, intercostal block.
Non-mechanical (spontaneous) pneumothorax can be primary or secondary. In the primary version, the lung ruptures during coughing, laughter, deep breathing due to congenital weakness of the pleura or disruption of the integrity of the bullae in patients with pulmonary emphysema. In healthy people, the cause may be a sharp change in external pressure when diving to depths during diving or flying at high altitude.
Secondary spontaneous pneumothorax is provoked by the melting of lung tissue during extensive pathological processes: abscess or gangrene of the lung, severe tuberculosis.
In case of pulmonary hemorrhage, infiltrative, cavernous and focal pulmonary tuberculosis, artificial pneumothorax may be applied. In this case, a certain amount of gas is specially introduced into the pleural cavity in order to achieve compression of the bleeding vessels or to provide more favorable conditions for the healing of tuberculosis foci.
Pathogenesis
The mechanism of development of pneumothorax is associated with the difference in pressure in the chest and the external environment. Normally, the pressure in the pleural cavity is below atmospheric, and in the lungs it corresponds to atmospheric pressure. Due to this, the lungs are in a straightened state. When air from outside or from other organs enters the pleural cavity, internal pressure increases, the lung contracts and stops working.
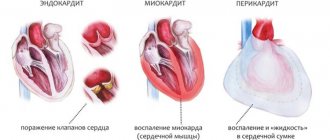
Classification
Taking into account the characteristics of the connection with the environment, 3 types of pneumothorax are distinguished:
- Closed . The most favorable option. A small amount of air enters the pleural cavity, the lung remains partially expanded.
- Open . The communication with the external environment is maintained. Gas continues to flow until the internal and external pressures are equal. The lung on the side of the injury completely collapses and is switched off from the act of breathing.
- Valve . Due to the nature of the hole, air flows in with each breath, but does not come out. The pressure continues to rise, exceeds atmospheric pressure, causing a sharp displacement of the mediastinal organs, compression of large vessels. Against the background of irritation of the pain receptors of the pleura, pleuropulmonary shock develops.
Depending on the volume, limited (partial, partial) and total (complete) pneumothorax are distinguished. Taking into account the prevalence, a distinction is made between unilateral and bilateral lesions. The larger the volume of the lung is excluded from the act of breathing, the more pronounced the respiratory disorders are - from shortness of breath with a limited variant of the pathology to suffocation and rapid death of the patient with complete bilateral pneumothorax.
Emergency care for pneumothorax
Pneumothorax in valvular or open form is one of the emergency conditions, the occurrence of which should immediately call an ambulance. Then be sure to do the following:
- stop the process of filling the victim’s pleural cavity with air;
- stop bleeding.
You will need to apply a tight, airtight bandage. In an emergency situation, in the absence of sterile equipment, you need to use improvised things - a shirt, a T-shirt. The cleanest area is applied to the wound. To seal the wound, a plastic bag (oilcloth, film) is placed over the improvised bandage.
You should also simplify the breathing process for the patient, for which he needs to be placed in an elevated position. All actions are carried out with extreme caution, as they cause additional pain to the victim. If a person faints, it is imperative to revive him. If ammonia is not on hand, any product with a strong odor will do, for example, gasoline, perfume, or nail polish remover. The product is applied to the nose.
The last task is to prevent the development of painful shock; banal aspirin or analgin will help with this. After providing first aid, you should wait for the ambulance to arrive.
Symptoms
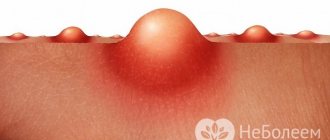
Photo: medicalnewstoday.com
Closed pneumothorax
Manifestations depend on the type and prevalence of the pathology. When the lung is compressed by less than 30-40%, specific symptoms may be absent or mildly expressed; the clinical picture is determined by the underlying disease. With more severe lesions, the patient complains of lack of air, acute chest pain, intensifying during inspiration. Typical symptoms are panic fear of death and paroxysmal dry cough.
Breathing is rapid, shallow, shortness of breath and tachycardia are detected. The skin and mucous membranes are pale, sometimes with a bluish tint. On auscultation of the affected half of the chest, breathing is weakened or not heard. During percussion, a box sound is detected. If air penetrates not only into the pleural cavity, but also into the superficial soft tissues, subcutaneous emphysema is detected. The surface of the chest looks swollen, and a gentle crunch is detected by palpation.
Open pneumothorax
Determining pathology is usually not difficult. The victim tries to stop the gas from entering the chest by lying on the sore side and pressing the wound. During inhalation, a whistling sound of air being sucked into the chest is heard. The blood in the wound is foamy due to mixing with gas. With puncture wounds with a narrow wound channel, the hole may be blocked by tissue and blood clots. In this case, the clinic will resemble a closed pneumothorax.
Spontaneous pneumothorax
Patients complain of a sharp stabbing pain that appears suddenly after laughing, coughing, taking a deep breath, or physical activity. The pain radiates to the neck and arm, intensifies with any movements, including chest excursions. After some time, the severity of shortness of breath and pain decreases. Subcutaneous emphysema may be detected in the chest, face and neck area. With a small amount of air, the symptoms of spontaneous pneumothorax are not clearly expressed.
Valvular pneumothorax
The patient's condition is extremely serious. The patient is agitated and complains of extremely intense stabbing pain in the chest. Shortness of breath, weakness, and bluish discoloration of the skin rapidly increase. The neck veins swell. Due to widespread emphysema, the face becomes moon-shaped, the shoulders and chest visually “swell,” and speech acquires a nasal tone.
Blood pressure is reduced, pulse is increased. Breathing is frequent and shallow. The affected side of the chest looks more healthy, the intercostal spaces are widened. Possible disturbances of consciousness. With the development of pleuropulmonary shock, shortness of breath intensifies, hypotension worsens, tachycardia gives way to bradycardia due to irritation of the vagus nerve. Sometimes the pulse remains frequent, but becomes barely noticeable. In the absence of medical care, death occurs.
Complications
Complications occur in half of pneumothorax cases. A serious early negative consequence is acute respiratory failure. In patients with trauma, hemothorax is often observed; in patients with purulent processes, pleural empyema is possible. During the recovery period, exudative pleurisy may develop. In the long term, adhesions form, preventing the free movements of the lung.
Kinds
Pneumothorax of the lung can be closed or open. In the first case, depressurization of the respiratory system occurs due to penetrating wounds. Then air and gases enter the pleural area from the outside. In the second case, the tightness of the chest is not broken, but the pleura itself has a defect.
According to another classification, pneumothorax of the lung is divided into the following types:
- secondary (identified as a complication of pathology of a pulmonary or non-pulmonary nature);
- artificial (sometimes created by doctors to carry out certain manipulations necessary to treat or diagnose a patient);
- spontaneous (occurring unexpectedly, without any precursors or underlying obvious diseases).
Diagnostics
Photo: twitter.com
Pathology is determined based on external examination data and the results of imaging techniques.
- Physical examination . The patient takes a forced position to facilitate breathing. The skin is moist, cool, pale or cyanotic. Excursions of the chest on the affected side are limited, the intercostal spaces are widened. Dyspnea, tachypnea, and tachycardia are observed.
- Radiography . The best conditions for confirming pneumothorax are created when the patient is in an upright position and using a direct projection. The images visualize an area of clearing without a pulmonary pattern, a displacement of the mediastinum, and a low dome of the diaphragm.
- CT scan . A more sensitive and informative test used when radiographic findings are ambiguous. Detects small limited pneumothorax, allows you to differentiate between gas in the pleural cavity and large air cysts in emphysema, and is carried out to clarify the cause of spontaneous pneumothorax.
Laboratory tests for diagnosis are not informative. Determination of the blood gas composition and acid-base balance is carried out to assess the severity of the patient’s condition, to determine the need and scope of resuscitation measures in the presence of extensive lesions and chronic background lung diseases.
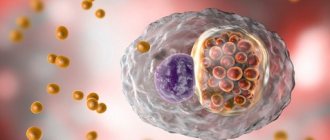
Treatment
Photo: canberraweekly.com.au
Pneumothorax is a life-threatening condition that requires emergency hospitalization in the traumatology or pulmonology department. Before the ambulance arrives, air access should be provided and the patient should be helped to take a comfortable position. If there is a wound, you need to seal the hole hermetically with a multi-layer gauze cloth with a piece of polyethylene placed on top.
Immediately upon admission, the patient is transported to the manipulation room or operating room, where, in case of a small pneumothorax, a pleural puncture is performed, and in case of a significant one, a drainage is applied. A puncture or incision to insert drainage is made in the second intercostal space at the level of the midclavicular line. The pressure in the pleural cavity is restored gradually to avoid shock from too rapid expansion of the lung.
In patients with open pneumothorax, the wound is sutured. In the valvular variant of the pathology, intrapleural pressure is reduced using a thick needle. Then treatment is carried out according to the scheme presented above. If the above methods are ineffective, a thoracotomy is performed to eliminate the cause of the pathological condition.
Prevention
Relapses are observed within 3 years after the first spontaneous pneumothorax in approximately 50 cases out of 100. The pathology in question is prevented by using video-assisted thoracoscopic surgery, during which bullae are sutured, pleurodesis, parietal pleurectomy or talc is administered. Some hospitals still perform thoracotomy today. These procedures are suitable when there is no effect of drainage of the pleural cavity in spontaneous pneumothorax, in recurrent pneumothorax, or in patients with secondary spontaneous pneumothorax. After this, recurrences of the pathology occur only in 5 cases out of 100. If thoracoscopy is not possible, chemical pleurodesis can be performed through a chest tube. This procedure is considered less invasive.
Medicines
Photo: zmina.info
Drug therapy plays a supporting role in the treatment of pneumothorax. In addition to the measures listed above, the following applies:
- Analgesics . In the first days after admission, they are administered intramuscularly. Depending on the intensity of pain, non-narcotic (analgin and analogues) or narcotic drugs are used. After reducing the severity of the pain syndrome, they switch to tablet forms of non-narcotic drugs.
- Local anesthetics . They are administered during cervical vagosympathetic blockade. Reduce pain, increase blood pressure, improve vascular tone, eliminate the cough reflex.
- Antibiotics . Necessary for open injuries and purulent processes. First, broad-spectrum medications are used. After receiving the results of the microbiological study, the antibiotic therapy regimen is adjusted taking into account the sensitivity of the pathogen.
- Bronchodilators . Indicated during the recovery stage to improve drainage of the bronchial system, prevent stagnation of sputum and the development of pneumonia.
An important role in the prevention of complications is played by breathing exercises, which are carried out from the first days of the patient’s stay in the hospital.
Consequences of the disease
Any serious illness limits a person's capabilities for some time, even after adequate treatment. A period of rehabilitation after pneumothorax is also necessary for the patient’s recovery. Upon completion of therapy and the patient’s discharge from the hospital, the doctor gives him the following recommendations:
- Completely eliminate smoking, including smoking mixtures, pipes, hookahs, electronic cigarettes, etc.;
- Avoid heavy physical activity for a month: a man should not lift more than 5-7 kg, and a woman – 3 kg;
- For 4 weeks, it is necessary to exclude any sudden changes in pressure: parachute jumping, diving, air travel, some attractions;
- Every 3 months, for a year, the patient should consult a pulmonologist and have spirometry performed. X-ray control every year;
- It is recommended to begin professional sports after pneumothorox no earlier than 3 months after recovery.
Folk remedies
Pneumothorax is a serious pathological condition that poses a danger to the life and health of the patient. Attempts at self-treatment using folk remedies and pharmaceutical drugs can lead to the death of the patient or the development of serious complications. If you suspect the development of this disease, you should immediately call an ambulance or take the victim to a specialized medical facility.
The information is for reference only and is not a guide to action. Do not self-medicate. At the first symptoms of the disease, consult a doctor.
How to make an appointment with a pulmonologist?
If you have symptoms of pneumothorax, you should visit a pulmonologist. The doctor will prescribe a diagnosis, conduct an examination and select treatment. Providing assistance for pneumothorax is extremely important, as it can cause the death of the patient.
To maintain your health and get the maximum chance of a quick recovery without consequences, visit JSC “Medicine” (academician Roitberg’s clinic) in the Central Administrative District of Moscow. We are located at: 2nd Tverskoy-Yamskaya lane, building 10. Just a 5-minute walk from Mayakovskaya metro station. You can also get to us from the Belorusskaya, Novoslobodskaya, Tverskaya, and Chekhovskaya metro stations.
Contact phone number for consultations and pre-registration: +7 (495) 995-00-33. If there is an urgent need for first aid for pneumothorax, you can call the emergency team by calling +7. Calls are accepted 24 hours a day.