© Author: Sazykina Oksana Yuryevna, cardiologist, especially for SosudInfo.ru (about the authors)
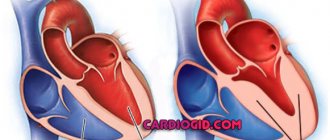
The right ventricle is a chamber of the heart that carries out the function of transmitting blood from the cavity of the right atrium to the mouth of the pulmonary trunk. This blood stream contains virtually no oxygen, but red blood cells contain large amounts of carbon dioxide. Next, the flow of venous blood is directed to the vessels located in the pulmonary tissue, from where it again flows to the heart (into the cavity of the left atrium). Thus, the right ventricle takes part in the formation of the pulmonary circulation.
Right ventricular hypertrophy is always a pathological condition, in contrast to the thickening of the left ventricle, which is often found in athletes and in this case is physiological. The term “hypertrophy” means an increase in the mass and thickness of the heart muscle; in other words, hypertrophied means large, enlarged. Right ventricular hypertrophy occurs when it is overloaded with pressure or volume .
- In the first case, blood has difficulty passing into the pulmonary vessels due to increased blood pressure in them, which makes it harder for the right ventricular muscle to push blood through than under normal conditions.
- In the second case, an additional discharge of blood occurs into the cavity of the right ventricle, due to which the wall of the ventricle is overstretched by the increased volume of blood.
In both cases, the right ventricle has to perform a greater load than before, so the heart muscle increases its mass. Hypertrophy of the myocardium of the right ventricle of the heart develops. Hypertrophy of the anterior wall of the right ventricle is more common.
RV hypertrophy is dangerous because sooner or later the heart muscle will not be able to work under high load conditions and the patient will begin to develop chronic heart failure.
The mechanism of formation of pancreatic hypertrophy in bronchopulmonary pathology is due to increasing pulmonary hypertension. As a result, pressure overload of the pancreas occurs. The development of pulmonary hypertension, or increased blood pressure in the lumen of the pulmonary arteries, in turn, occurs due to a decrease in the elasticity of the lung tissue.
The mechanism of pathology development
The pathogenic process is formed in several stages. In any case, the basis is an increase in blood pressure. This is not an axiom, there is another option.
As blood pressure rises, a change occurs in the entire bloodstream. Liquid connective tissue is thrown into the chambers with great force.
The impact also occurs on the mitral valve, but the right ventricle takes the main blow.
This chamber is responsible for the release of blood into the small or pulmonary circle.
As a result of the influence of certain factors, the vessels narrow and resistance increases.
The body compensates for the condition by intensifying contractions and greater force of blows. The heart, unable to work in this mode for a long time, builds muscle mass.
Due to the proliferation of new cardiomyocytes (active heart cells), an anatomical defect occurs - hypertrophy. If it is isolated, there is no significant difference in functional activity.
The second option is excess volume. If there is a lot of blood coming in, the heart cannot adequately pump it around the body.
Dilation occurs (expansion, enlargement of the chamber) and proliferation of the myocardium, as a compensatory mechanism. This condition occurs mainly in athletes and manual workers.
Types of hypertrophy
Based on the mechanism of development of the pathological process, two forms of deviation are distinguished. They have already been named.
- The first is hypertensive. The essence is an increase in pressure, narrowing of blood vessels, including the pulmonary arteries. Blood does not flow in sufficient quantities due to the resistance of the stenotic (narrowed) hollow structures. Hence the need for greater blood pressure to push an adequate volume into the channel.
Symptoms of this form develop almost immediately: shortness of breath, rhythm disturbances, chest pain.
However, episodic manifestations. Only in the later stages do they stabilize and haunt the person constantly.
- The second is dilation. A combined process arises. On one side, the right chamber stretches, increases in volume and fills with blood. Hence the increase in pressure at the local level. The further scheme is identical.
Regardless of the form, the condition will require mandatory treatment.
Attention:
RVH is the first step towards heart failure. Once it develops, it is no longer possible to radically help. The likelihood of death increases dramatically.
Differences between different types of LVH
Cardiomyopathy | Arterial hypertension | Sports heart | |
| Age | under 35 | over 35 | from 30 |
| Floor | both sexes | both sexes | more often men |
| Heredity | burdened with hypertension | burdened with cardiomyopathy | not burdened |
| Complaints | dizziness, shortness of breath, fainting, heart pain, rhythm disturbances | headaches, less often shortness of breath | stabbing pain in the heart, bradycardia |
| Type of LVH | asymmetrical | uniform | symmetrical |
| Myocardial thickness | more than 1.5 cm | less than 1.5 cm | decreases when the load stops |
| LV dilatation | rarely, more often a decrease | Maybe | more than 5.5 cm |
Causes
Numerous, almost always pulmonary, less often vascular and cardiac. But not all are pathogenic.
Sports activities
The first and most pronounced factor is long-term sports at a professional or amateur level. Not just activity, but grueling training to the limit.
If you look at the Borg scale, it’s 7-10 points. Essentially wear and tear on the body.
The body is not adapted to such extreme overloads. The heart responds accordingly with a dilated form of right ventricular hypertrophy.
The body has its own margin of safety, relatively speaking. Having crossed a certain line, it cannot perceive activity at the same level. Possible heart attack, dangerous arrhythmia, acute asystole.
Manual workers are also at risk, but not to the same extent. In any case, the question of the possibility of continuing this lifestyle is decided at an appointment with a cardiologist after diagnosis.
Pneumonia
Especially with frequent relapses. Another name is pneumonia. Develops as a result of damage by bacteria, less often by viruses.
There is a narrowing, then destruction and scarring of active tissues. The vital capacity of the lungs decreases, hence respiratory failure. A small amount of oxygen leads to increased pressure in the artery of the same name.
And further along the chain: all the vessels of the small circle suffer, they become stenotic and narrow. This leads to an increase in pressure in the right ventricle, and the tissues grow.
A one-time disease, especially in the acute phase, can result in cor pulmonale, but persistent anatomical defects are extremely rare.
Chronic obstructive disease (COPD)
The development pattern is approximately the same. With one exception - this diagnosis is made once and for life. Treatment helps correct the condition, but does not eliminate it.
Sooner or later, patients begin to develop cardiovascular problems.
Since many people turn to a pulmonologist after many years of stable progression of COPD, a whole bunch of diseases of different profiles are diagnosed.
The main contingent of patients are heavy smokers and workers of hazardous chemical, textile, and metallurgical enterprises.
Bronchiectasis
Formation of pus-filled cavities - “bags”. After opening, including as part of treatment, they disintegrate. Large tissue defects remain, shaped like tuberculosis cavities.
Emphysema
It is similar in nature to the previous process. Only a pathological expansion of the alveoli occurs, their rupture and the formation of cavities that do not participate in normal activity.
It is also impossible to help radically. Lifelong maintenance therapy is required.
If started early, the prognosis is good. The main contingent is the same - smokers, workers in hazardous industries.
Asthma
Usually of allergic origin. Rapid narrowing of the bronchi due to exposure to a negative factor. The quality of breathing decreases, gas exchange worsens.
Advanced forms are not fully controlled even with hormonal drugs. Attacks occur several times a day, including at night.
Persistent respiratory failure of degrees 1-3 develops. The pressure in the pulmonary artery and pulmonary vessels increases.
The right ventricle enlarges, CPS (chronic cor pulmonale) is diagnosed. In rare cases - acute form.
Cystic fibrosis
A chronic condition affecting the digestive tract as well as the lungs.
All diseases of the respiratory system are characterized by one phenomenon, common in symptoms. It is characterized by a stable increase in pressure and a change in cellular structure.
We're talking about cor pulmonale. Acute rarely leads to visible defects in the organ. Chronic pathology is much more dangerous.
Heart defects
Congenital defects of cardiac structures are represented by a group of disorders, for example, tetralogy of Fallot and others. As a rule, patients with severe abnormalities in heart development die within the first year without urgent treatment, sometimes faster.
Acquired defects are much more common. For a long time they do not produce symptoms and remain unnoticed until the last moment.
The diagnosis can be made based on the results of an autopsy (autopsy). If you're lucky, earlier, when cure is still possible. Therefore, it is recommended to undergo regular preventive examinations.
Mitral valve insufficiency is a special case. Accompanied by reverse blood flow or regurgitation.
Disturbances in the functioning of the tricuspid valve (three leaflets) affect approximately the same way, but cause hypertrophy of the right ventricle more often.
It is extremely rare that tumors are the culprits of the defect. The heart itself or the respiratory organs. They are easily determined by the results of a simple x-ray or echocardiography. It is already more difficult to say about the histological structure; a biopsy will be required.
Symptoms
Signs of HPV are relatively easy to identify. But they are nonspecific, therefore they are associated with a lot of conditions, and differential diagnosis is required. It’s impossible to say anything for sure based on signs alone.
The clinical picture includes:
- Regular chest pain. The intensity is minimal. The discomfort is burning, pressing. They resemble angina, but are weaker and last longer.
- Tachycardia. Heart rate varies from 100 to 150 beats per minute. Sinus type, paroxysms are extremely rare. There is a possibility of atrial fibrillation, which significantly worsens the prognosis and indicates the onset of heart failure.
- A drop in blood pressure followed by an increase. The level is unstable. The assessment is carried out over time.
- Cough. Dry, unproductive. A small amount of blood may be released. An alarming sign. Requires mandatory differential measures, since we may be talking about a tuberculosis process.
- Dyspnea. Decreased exercise tolerance. The patient is unable to walk normally, let alone play sports. The disturbance is observed even at rest.
- Fatigue, drowsiness, weakness for no apparent reason. The patient is unable to perform daily activities. Over time, a once healthy person without treatment turns into a deeply disabled person.
These symptoms are accompanied by signs of the underlying process itself. Against the background of bronchopulmonary pathologies, suffocation, impaired gas exchange of an objective nature (decrease in the level of oxygen saturation in the blood), cough, whistling, and wheezing are noted.
Thickening of fingers and nails is possible. Pallor of the skin, cyanosis of the nasolabial triangle.
Against the background of hypoxia (oxygen starvation), fainting develops, often repeatedly. Headaches, vertigo, and inability to navigate in space should alert the patient and his doctor - this is a direct indication of cerebral ischemia.
There is a high probability of a stroke. It is difficult to say in what time frame; it is necessary to evaluate all factors: from age to the moment of development of pathology. Read about the signs of a pre-stroke condition here.
Features of right ventricular hypertrophy in children
This condition in childhood is most often caused by congenital heart defects, such as tetralogy of Fallot, congenital pulmonary stenosis and idiopathic pulmonary hypertension. At the time of birth, a thickening of the pancreas wall may already be formed, but more often it develops in the first months of life. Clinically, pancreatic hypertrophy is manifested by cyanosis, swelling of the jugular veins, lethargy, or, conversely, severe anxiety in the infant. In addition, the child experiences severe shortness of breath and bluish skin when sucking on a breast or bottle, as well as during physical activity or restlessness, or when crying.
Diagnosis of hypertrophy is not difficult thanks to the active implementation of cardiac ultrasound in newborns. If the defect is not diagnosed by ultrasound during pregnancy or immediately after childbirth, then the type of defect, as well as the presence/absence of hypertrophy, is established within 1 month after birth, since in recent years, screening examinations of infants include mandatory echocardioscopy.
Treatment of hypertrophy in a newborn is carried out strictly under the supervision of a pediatric cardiologist and cardiac surgeon, who determine the timing and tactics of surgical intervention for the defect.
Diagnostics
It is carried out under the close supervision of a cardiologist. It is possible to involve a specialist pulmonologist, a doctor to identify and treat pathologies of the bronchi and lungs, and the respiratory system as a whole.
An approximate list of activities consists of the following components:
- Oral survey regarding complaints. When did it arise, how much does it interfere, are there any breaks in the clinic?
- Anamnesis collection. Lifestyle, bad habits, past pathologies, current diseases, nature of professional activity, leisure time and other points.
- Measurement of blood pressure, heart rate. Using routine methods.
- 24-hour Holter monitoring. Using a special programmable device with sensors, pulse and blood pressure are recorded. In 24 hours. It is better if the patient is in a familiar environment, at home or at work. This will help detect deviations much more accurately.
- Electrocardiography. Study of the functional status of the heart. Used as a second method. Gives an idea about arrhythmias.
- Echocardiography. Used to identify anatomical disorders. The main method of early diagnosis or determination of the severity of the disease.
- Spirography. The respiratory function is subject to assessment, that is, how much the ability of the entire system to adequately operate is preserved. For a more accurate result, it is carried out with a sample of drugs like Salbutamol (with a load).
- Auscultation. Listening to heart sounds.
- X-ray of the chest organs.
- MRI of the same area. CT is often used to verify problems with pulmonary structures.
It is possible to prescribe a general blood test, biochemistry, and hormonal tests. As needed.
Attention:
Fluorography cannot replace x-rays, so doctors offer it for routine detection of gross, advanced defects. This is more of a formality than a real diagnosis.
Is it possible to cure pancreatic hypertrophy forever?
In the treatment of pancreatic hypertrophy, it is necessary to understand the following point - it is easier to prevent the development of hypertrophy than to treat its complications. That is why any patient with a pathology of the bronchopulmonary system or a heart defect needs successful treatment of the underlying disease. Thus, for bronchial asthma, the patient should receive basic therapy (continuous use of inhaled drugs such as Spiriva, Foradil Combi, Seretide and others prescribed by a doctor). The key to successful treatment of pneumonia and prevention of its relapse is well-chosen antibacterial therapy, taking into account sputum culture for flora and its sensitivity to antibiotics. In case of COPD, the patient must eliminate the harmful effects of tobacco and harmful occupational factors on the bronchi as soon as possible.
Patients with heart defects require surgical correction if the cardiac surgeon has determined the indications for surgery during an in-person examination.
When severe hypertrophy develops and chronic heart failure develops, the patient is advised to take long-term or constant use of the following medications:
- Diuretics (furosemide, indapamide, veroshpiron) - by acting on the renal tubules, they remove “excess” fluid from the body, making it easier for the heart to pump blood.
- ACE inhibitors (enam, diroton, prestarium, perineva) significantly slow down the processes of myocardial remodeling and slow down the progression of cardiac muscle hypertrophy.
- Nitroglycerin preparations (monocinque, nitrosorbide) - reduce the tone of the pulmonary veins, thus reducing the preload on the heart muscle.
- Calcium channel inhibitors (verapamil, amlodipine) help relax the heart muscle and reduce heart rate, which has a beneficial effect on myocardial contractility.
In any case, such nuances as the nature, quantity and combination of drugs, as well as the frequency and duration of their administration are determined only by the attending physician after a full examination of the patient.
Unfortunately, pancreatic hypertrophy does not regress back, but it is possible to prevent its rapid growth, as well as decompensation of heart failure with the help of treatment, in almost all cases, provided that the underlying disease is successfully treated.
Signs on ECG
The features on the cardiogram are:
- Change in the width of the QRS complexes, its significant deformation. Especially in leads V1, V6.
- Incorrect placement of STV1, 6, SV1, 6 segments.
Changes can be detected in this way only in moderate and severe forms of the pathological process. The technique is not suitable for early diagnosis due to insufficient information content.
However, signs of right ventricular hypertrophy on the ECG are taken into account and compared with the results of echocardiography.
If there is a significant discrepancy, they focus on the worst option and make a diagnosis based on it. But then you need to re-evaluate the condition; perhaps a mistake was made.
conclusions
The right ventricle determines the functional state of the pulmonary circulation, on which tissue oxygen saturation depends. Problems with the functioning of the pancreas are often associated with diseases of the respiratory or cardiovascular system. The appearance of signs of stagnation is a reason to contact a therapist or cardiologist. Modern medicine offers many safe and informative methods for diagnosing pathologies in the first stages. Early initiation of treatment prevents the development of complications and progression of the disease.
Treatment
Carried out by a group of methods. The basis is eliminating the root cause. Medicines are usually used. Which ones exactly depend on the diagnosis.
Basic therapy is required against the background of bronchopulmonary problems; the issue of selecting medications is decided by the doctor, since there are a lot of options.
As for the symptomatic measure, it is aimed at relieving manifestations and preventing dangerous complications.
What drugs are used to treat:
- ACE inhibitors. Like Prestarium and its analogues. Help eliminate excess pressure in the bloodstream.
- Calcium antagonists. Verapamil, Diltiazem, others with great caution.
- Centrally acting medications. Moxonidine.
- Nitroglycerin to relieve attacks. It is possible to use analogues in the group.
- Cardioprotectors. Mildronate and others. To restore metabolic processes.
- Diuretics as needed. These products are not suitable for continuous use.
Surgical treatment is rarely indicated to eliminate anatomical defects and defects. The issue is decided at the discretion of the practicing operating cardiologist.
If right ventricular hypertrophy occurs as a result of long-term grueling physical training, a significant reduction in the intensity of exercise is indicated.
Although this is a physiological variant of the deviation, its naturalness is very conditional. With further progression, which will inevitably happen, the patient's death is likely. GPG is the basis for exclusion from professional and even amateur sports.
General recommendations
In addition to medical prescriptions, preventive measures must also be followed. During heart disorders, the following recommendations will be extremely useful:
- Avoid drinking alcohol, which has a toxic effect on the heart muscle.
- Exclusion from the daily menu of products with high cholesterol content. This helps prevent the deposition of cholesterol plaques on the vascular walls. It is optimal to add fish, olive, flaxseed, corn and soybean oil to your diet at least twice a week.
- Inclusion in the menu of such products as viburnum, cranberries, cabbage, eggplants, apples, pomegranates, etc. They will help strengthen and maintain the myocardium in proper condition.
- Salt intake should be limited to 2 g per day, in particular for patients with high swelling.
- When obesity is diagnosed, a proper balanced diet should be formulated that aims to eliminate those extra pounds.
- The duration of sleep should be at least 8 hours, avoiding physical and psycho-emotional fatigue.
- Frequent walks in the fresh air.
Cardiac enlargement is not a diagnosis, but only a temporary condition of the myocardium. With proper and timely treatment of this pathology, it is possible to eliminate the disease and significantly improve the patient’s condition.
Forecast
Depends on the diagnosis. Against the background of potentially incurable pulmonary conditions, the likelihood of complete recovery is minimal. But you can take control of the disease.
Symptomatic and etiotropic therapy are associated with high survival. The risk of death is about 7%, approximately 1-3% during supervision, which is quite small, considering the essence of the pathological process.
If heart failure begins, the outcome worsens significantly. The probability of death is 20-25% or higher.
Negative factors based on age, gender, physical condition, general history, family history, lifestyle, addictions, and other factors are taken into account.
The response to the treatment is also taken into account, and whether there is a possibility of radial intervention. As a result, a complex, systemic picture emerges. It will not be possible to average it; a qualified assessment by a specialist is needed.
About cardiomyopathies
Pathological processes in myocardial cells are based on hereditary predisposition (idiopathic cardiopathy) or dystrophy and sclerosis. The latter are caused by myocarditis, allergies and toxic damage to heart cells, endocrine pathologies (excess catecholamines and somatotropic hormone), and immune disorders.
Types of cardiomyopathies occurring with LVH:
Hypertrophic form
It may produce diffuse or limited symmetrical or asymmetrical thickening of the muscle layer of the left ventricle. At the same time, the volume of the heart chambers decreases. The disease most often affects men and is inherited.
Clinical manifestations depend on the severity of obstruction of the heart chambers. The obstructive variant gives the clinical picture of aortic stenosis: heart pain, dizziness, fainting, weakness, pallor, shortness of breath. Arrhythmias may be detected. As the disease progresses, signs of heart failure develop.
The boundaries of the heart expand (mainly due to the left sections). There is a downward displacement of the apical impulse and dullness of heart sounds. A functional systolic murmur is characteristic, heard after the first heart sound.
Dilated form
It is manifested by expansion of the chambers of the heart and hypertrophy of the myocardium of all its parts. At the same time, the contractile capabilities of the myocardium decrease. Only 10% of all cases of this cardiomyopathy occur in hereditary forms. In other cases, inflammatory and toxic factors are to blame. Dilated cardiopathy often manifests itself at a young age (30-35 years).
The most typical manifestation is the clinical picture of left ventricular failure: bluish lips, shortness of breath, cardiac asthma or pulmonary edema. The right ventricle also suffers, which is expressed in cyanosis of the hands, enlarged liver, accumulation of fluid in the abdominal cavity, peripheral edema, and swelling of the neck veins. Severe rhythm disorders are also observed: paroxysms of tachycardia, atrial fibrillation. Patients may die due to ventricular fibrillation or asystole.
Hypertrophy of the left ventricular myocardium is diffuse. The expansion of the cardiac cavities prevails over the thickening of the myocardium. Learn more about the symptoms and treatment of cardiomyopathy.
Possible complications
Among the consequences:
- Heart failure. As a result of overload and the development of dangerous forms of arrhythmia.
- Heart attack. Death of active cells of cardiac structures. If the patient does not die, coronary heart disease occurs, which at a minimum significantly worsens the quality of life.
- Stroke. Necrosis of cerebral structures with the formation of a persistent neurological focal defect. Death is also possible, depending on the extent of the lesion and location.
- Vascular dementia.
- Pulmonary edema.
- Asthma.
Preventing dangerous complications is perhaps the main goal of treatment. Because it is these consequences that lead to death.
Hypertrophy of the right ventricle of the heart is the result of bronchopulmonary pathologies or defects of cardiac structures, less often the own achievement of a patient with sports merits.
Despite the relatively favorable prognosis, we cannot relax. Without treatment, the condition develops into a deficiency, which is almost guaranteed to lead a person to the grave sooner or later.
Prevention
To prevent the appearance of hypertrophic processes in the right ventricle, it is necessary to engage in the prevention of pulmonary pathologies:
- avoid drafts;
- eliminate smoking;
- do not overcool;
- apply oxygen therapy;
- exercise;
- promptly treat viral infections of the respiratory organs.
Hypertrophic damage to the right ventricle often provokes negative health consequences. To minimize the risk of dangerous complications, it is necessary to contact a cardiologist in a timely manner and strictly adhere to his recommendations.
Did you like the article? Save it!
Still have questions? Ask them in the comments! Cardiologist Mariam Harutyunyan will answer them.
Ivan Grekhov
Graduated from the Ural State Medical University with a degree in General Medicine. General practitioner