Under the influence of hormones, eggs (female reproductive cells) develop and mature in the gonads.
Under the influence of various factors, a follicular ovarian cyst develops in the ovary, which is a functional formation that can regress on its own without special treatment and in most cases does not give characteristic symptoms. Functional cysts belong to benign tumor-like processes; they are classified by location and are formed predominantly on one side.
Therefore, it may occur:
- follicular cyst of the left ovary;
- follicular cyst of the right ovary.
Bilateral cystic formations are extremely rare. Conventionally, according to the course of the pathological process, cystic formations can be divided into complicated and uncomplicated.
What is a follicular cyst
Every month, a woman’s body undergoes hormonal changes. With the beginning of the next menstrual cycle, the active production of follicle-stimulating hormone begins, which is responsible for the maturation of the egg.
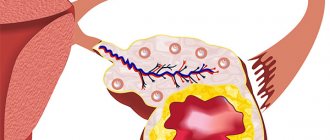
In the ovarian cavity there are many primordial follicles, ready for gradual development. Of these, only one (rarely two) matures to the formation of a graafian vesicle.
Timely production of LH provokes the opening of the dominant follicle, as a result of which a mature and ready-for-fertilization egg enters the abdominal cavity. If for some reason the Graafian vesicle does not open, then a follicular ovarian cyst is formed.
Important! A follicular cyst is a small benign neoplasm located in the ovary. Its size usually does not exceed 7–10 cm. The share of all ovarian tumors accounts for up to 80% of follicular tumors. The peculiarity of such a neoplasm is that it will never turn into a malignant form.
The neoplasm has a single-chamber or two-chamber structure, and inside it there is a fluid accumulation saturated with estrogen. Despite the ease of diagnosis, functional tumors are rarely identified.
About 70% of patients are unaware that they have ever had a similar problem. The uniqueness of the neoplasm lies in the possibility of reverse transformation and the tendency to disappear.
Left
Follicular cyst of the left ovary occurs quite rarely. This gland is supplied with blood through the renal artery. As a result of the greater passage of the blood path from the heart, Graafian vesicles on the left mature less frequently, which reduces the likelihood of a tumor appearing here.
This pattern is a medical observation and does not guarantee the absence of tumors in the left gland throughout life.
For the left ovary, the reasons for the appearance of a neoplasm are no different from the right. The appearance of the tumor is primarily due to hormonal imbalances. Only a doctor can determine what caused the formation of a large, unopened Graafian vesicle.
Right
The right side has a different power supply system than the left. This gland is inextricably linked with the aorta. Improved blood supply causes increased follicle maturation.
This pattern explains that follicular cysts of the right ovary are found more often in women.
Another feature is the size of the tumor. The average cyst on the right has a larger volume than tumors on the gland located on the left.
The mechanism of development of a functional neoplasm on both sides is no different. Despite statistical data, the likelihood of tumor formation in the right and left glands remains in all representatives of the fair sex during reproductive age.
What do normal ovaries look like during ultrasound examination?
Normally, during an ultrasound examination, both ovaries are almost the same size:
- length – 30-41 mm;
- width – 20-31 mm;
- thickness – 14-22 mm;
- volume – about 12 cubic ml.
Due to the maturing follicles, the surface of the organ looks bumpy. Since the ovary is well supplied with blood, its tissues contain many blood vessels.
Typically, at least 12 cells mature in two ovaries. Among them stands out a dominant follicle measuring 10-22 mm, from which an egg will be released in the middle of the cycle. If ovulation has already passed, the corpus luteum is visible inside the ovary, secreting hormones necessary for implantation and development of the embryo. If conception does not occur, the corpus luteum dissolves.
Causes
It is believed that ovarian follicular cysts occur due to hormonal imbalances. The reasons for unstable changes may be:
- inflammatory and infectious diseases of the genital organs;
- puberty or menopause;
- hormonal treatment;
- self-administration of oral contraceptives;
- stress and emotional distress;
- ovarian dysfunction;
- endocrine disorders.
Important! The absence of ovulation in a healthy woman for 1-2 months per year is normal. Therefore, diagnosing 1-2 cases of the formation of an overgrown and unopened follicle is not a cause for concern.
With the development of medicine, specialists found new reasons for the appearance of functional neoplasms. Back in the 19th century, it was assumed that the tumor appears only in nulliparous women after 40 years of age. Then the disease was called dropsy.
Over time, a hypothesis was put forward that a woman’s body self-destructs cells at the genetic level. Modern medicine recognizes that the cause of tumors is not only hormonal disorders.
A follicular neoplasm can grow due to excessive blood supply to the gonad, which in turn occurs due to inflammation, benign or malignant tumors and other unnatural processes in the pelvis.
Kinds
There are 2 main types of follicular type tumors:
- single-chamber. Outwardly, it looks like a round bubble without partitions in the middle. Such a cyst is found in 95% of cases;
- two-chamber. Outwardly it resembles 2 separate tumors that are pressed tightly against each other. It occurs when two dominant follicles mature at once, so it is quite rare.
The treatment method is selected after determining the type of tumor.
Symptoms of a follicular cyst
Small neoplasms reaching a maximum size of 4 cm are characterized by an asymptomatic course. An important role is played by the sensitivity and pain threshold of the patient. The same tumor may present differently in individual women. Large neoplasms reaching a size of 6 cm or more are accompanied by the following clinical signs:
- prolonged and unusually heavy menstrual bleeding;
- delay of menstruation and lengthening of the cycle;
- pain and a feeling of fullness in the lower abdomen (right or left, depending on the location of the bubble);
- changes in hormonal levels.
One of the reliable signs of cystic formation is the absence of ovulation. Women who measure their basal temperature and keep a chart can independently determine this indicator.
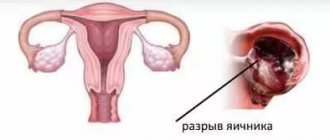
The rupture of a follicular ovarian cyst becomes a clear symptom of pathology, developing as an “acute abdomen”.
Signs of torsion
Torsion of a cystic follicle is a condition in which the tumor stretches out, forming a stalk, and turns in the other direction. In such a situation, a malnutrition of the tumor occurs, which is where tissue necrosis begins.
This complication rarely develops. Excessive physical activity, sexual contact and other factors become a provocateur.
Signs that the tumor vesicle has become twisted cannot be ignored. The pathological condition is accompanied by strong cutting sensations that cannot be tolerated even with a high pain threshold.
The woman turns pale and sweat appears on her face. An additional clinical sign will be a decrease in blood pressure.
Gap
Rupture of the cystic capsule is characterized by a clear clinical picture. The patient feels pain on the side of the abdomen where the tumor is located. Blood pressure decreases, fainting occurs.
Body temperature may rise to high levels. Vomiting and nausea occur due to the involvement of the digestive tract in the process. This may cause diarrhea or, conversely, constipation.
Against the background of low blood pressure, the patient feels increased heartbeat and increased pulse.
If the ovary ruptures along with the follicle (the capsule of the gland ruptures), then intra-abdominal bleeding develops. Bloody discharge from the genitals is also observed when a vessel located near the cystic neoplasm is damaged.
Clinical picture
The more actively estrogen hormones are produced, the brighter the signs of follicular formation will appear. They can also be aggravated by the presence of chronic gynecological diseases (adnexin, endometriosis, fibroids).
The most characteristic symptom of an ovarian cyst is a delay in menstruation, and the cycle can increase by 5 to 21 days, or even more. The presence of a follicular tumor can be determined by the following accompanying signs:
- nagging pain in the perineum with projection to the lower back and leg;
- frequent trips to the toilet;
- problems with the intestines (feeling of heaviness, bloating, diarrhea, constipation);
- intermenstrual bleeding;
- pain that intensifies closer to menstruation, after physical activity, intimacy, long walks and sudden movements.
If the size of the cyst does not exceed 4 cm and at the same time estrogen is actively produced, then it may not manifest itself in any way and often resolves on its own against the background of hormonal activity with the arrival of menstrual periods. If the tumor has reached 8 cm or more, the woman may have abdominal pain in the iliac fossa on the side of the affected ovary.
Since the symptoms of the cyst are nonspecific and similar to the signs of many gynecological pathologies, only a doctor can establish an accurate diagnosis after carrying out a series of diagnostic measures.
Symptoms of a rupture
Ovarian cysts rupture unexpectedly, often in the middle of the menstrual cycle during ovulation.
The cystic capsule, under the influence of hormones, grows together with the dominant follicle and when certain conditions are reached, it ruptures.
A woman can know that a follicular tumor has burst by the following symptoms:
- acute dagger-type pain from the affected ovary;
- Over time, pain subsides and becomes blurred;
- blood pressure and heart rate decreases;
- the stomach is tense;
- the woman breaks out in a cold sweat;
- nausea to the point of vomiting;
- loss of consciousness.
If the tumor is located near blood vessels, then if it ruptures there is a high probability of hemorrhage into the abdominal cavity. At the same time, the mucous membrane and skin turn pale, the pulse quickens and the pressure drops. This situation occurs in cases where the cyst grows rapidly and at the same time the patient suddenly changes her body position. Bleeding can only be stopped in a hospital setting.
Cyst torsion
After a fall, sudden movement or intimacy, torsion of the pedicle of the cystic neoplasm may occur, which is accompanied by compression of the neurovascular bundle of the gonad. The size of the cyst does not matter in this case.
Symptoms of torsion will be as follows:
- heart beats faster;
- an inexplicable feeling of fear arises;
- pressure drops;
- breaks into a cold sweat;
- the skin turns pale;
- nauseated to the point of vomiting;
- intestinal activity decreases;
- the temperature increases slightly;
- intense pain occurs from the affected ovary, which does not subside either when changing position or at rest.
To prevent such complications, it is necessary to diagnose the pathology in a timely manner and begin its treatment; in some cases, surgical intervention will be justified.
Diagnostics
Identifying a cyst is not difficult. It is enough to perform an ultrasound examination, which allows you to find out not only about the presence of a tumor, but also to determine its size.
Additional Doppler mapping, which establishes blood flow, will help to obtain more information about the tumor.
During a gynecological examination, as well as during a visual examination, it will not be possible to detect a cyst. If the tumor is large (from 6 cm), then it can be palpated.
Which doctor should I contact?
If you experience symptoms characteristic of the development of a follicular cyst, you need to make an appointment with a gynecologist. The doctor will conduct a survey, examine you, refer you to undergo the necessary examination, and, based on the diagnostic results, prescribe treatment. If the gynecologist determines that the appearance of a follicular cyst is caused by urogenital infections, the woman needs to make an appointment with a venereologist. When hormonal imbalance is caused by stress, you will need to consult a neurologist: a specialist will prescribe sedative (calming) drugs.
Choose a specialist, read reviews and make an appointment with a gynecologist online
How to treat a follicular cyst
Treatment of a follicular cyst is carried out only if it causes discomfort to the patient, is large in volume and does not go away on its own within three menstrual cycles.
Before taking measures aimed at eliminating the tumor, doctors choose a wait-and-see approach. In most patients, the resulting capsules undergo involution within 3-4 cycles.
If the reverse transformation does not occur, then the gynecologist selects hormonal therapy for a period of 3 to 6 months. When traditional methods fail, drastic measures are taken—surgical treatment.
The operation is performed as an emergency if pedicle torsion, capsule rupture, or ovarian apoplexy occurs.
Waiting method
It is assumed that functional neoplasms resolve on their own. If such a pathology is detected, doctors give the patient up to 3 months.
At the same time, ultrasound scans are carried out regularly to assess the dynamics of the tumor. Watchful waiting is chosen in case of asymptomatic pathology, as well as when the tumor size is no more than 5 cm.
If after 3 cycles the tumor has not resolved or has begun to increase in size, manifesting itself with clinical symptoms, then the attitude to treatment is reconsidered.
Use of medications
It is customary to treat ovarian cysts with hormonal agents. Therapy involves the prescription of oral contraceptives for a period of 6 months. It is expected that during this time the reproductive function will be preserved, and the neoplasm will undergo regression.
At the same time, the drugs will improve the woman’s hormonal levels, which will prevent the problem from recurring in the near future. After discontinuation of oral contraceptives, the chances of successful conception increase in the first 2-4 months.
Along with hormonal therapy, the patient is recommended to take vitamins that strengthen the immune system and non-steroidal anti-inflammatory drugs.
Physiotherapy
Clinical symptoms and treatment of a woman are interrelated (treatment of small tumors is prescribed when signs of pathology appear). A popular and safe method is physiotherapy.
Its effectiveness is noted in the presence of small tumors. Electrophoresis, magnetic therapy and other means are used when there is a tendency for tumor growth.
Laparoscopy
Treatment of follicular ovarian cysts that increase in size is carried out through laparoscopy.
The low-traumatic procedure involves making three punctures in the abdominal cavity, through which miniature manipulators are inserted. Depending on the condition of the affected gonad, one of the following methods is performed:
- cystectomy – removal of a tumor;
- resection - excision of an enlarged vesicle with removal of damaged tissue;
- Ovariectomy – thorough removal of the gland (performed for apoplexy).
Laparoscopy is performed under general anesthesia using a ventilator.
Surgical intervention
If the follicular ovaries have percussion or apoplexy, then laparotomy is performed - a strip surgical procedure that involves making an incision on the abdominal wall.
The procedure is quite traumatic and can be accompanied by various complications (from adhesions to heavy bleeding and death).
Laparotomy is usually performed when laparoscopy is not possible. One of the circumstances that can influence the choice of surgical treatment technique is obesity.
Psychological factor
It has long been known that the parts of the central nervous system - the hypothalamus and pituitary gland, located in the brain - are responsible for the functioning of the ovaries. It is assumed that a functional ovarian cyst can be cured through psychological influence.
When the patient uses the same parts of the brain (when thinking about a pressing problem, stress, nervous experiences), other functions fade away. This pattern determines the psychosomatic reasons for the appearance of an overgrown follicle.
In order to solve a health problem, you just need to switch. Some women may need to consult a psychologist for this.
During pregnancy
If a follicular type cyst is diagnosed, most often it develops against the background of lack of ovulation. Under such conditions, a woman’s ability to conceive is significantly reduced, since the egg matures only in a healthy ovary. In rare cases, infertility may develop. Due to complications of the pathology (torsions, ruptures, bleeding), the likelihood of miscarriage in the early stages greatly increases.
If the tumor was discovered during pregnancy, it can be removed laparoscopically in the 2nd trimester. This manipulation helps protect the expectant mother and fetus from severe complications that can be life-threatening.
Complications
For most patients, the prognosis for functional neoplasms is favorable. Complications and consequences should be feared with a tendency to growth and clinical manifestations of the tumor. Among the most dangerous are torsion and apoplexy.
Also, a large tumor that does not go away over a long period of time can cause infertility. The neoplasm can cause adhesions, which can also impair the functioning of the reproductive organs.
Forecast
Follicular-type cysts are prone to self-healing; most women may not even realize that at a certain stage of life such inclusions occurred in their ovaries. If you consult a doctor in a timely manner, the prognosis for full recovery is also favorable.
But the prognosis for the treatment of complications will depend on how quickly the woman consulted a doctor after the first symptoms. The earlier the operation was performed, the lower the risk of developing postoperative consequences and relapse of the pathology.
Prognosis and prevention
Due to the fact that many patients are unaware of their diagnosis and the tumor disappears on its own, the outlook is good. Even with the prescription of drug treatment, the prognosis remains favorable. Hormone therapy shows good results.
The prognosis for treatment of complications directly depends on the time of seeking medical help. The sooner the operation is performed, the better for the patient.
There is no specific prevention for the formation of functional ovarian cysts.
A correct lifestyle, moderate physical activity, maintaining natural hormonal levels (refusing to use medications on your own) and timely examination will help prevent the unpleasant consequences of pathology.
Sources
- Clinical recommendations. Obstetrics and gynecology /under. ed. IN AND. Kulakova.- M.: GEOTAR-Media, 2006. – 512 p. ill. ISBN 5-9704-0201-Х
- A. N. Strirzhakov, A. I. Davydov, L. D. Belotserkovtseva. Minimally invasive surgery in gynecology. – M.: “Medicine”, 2001. – 221 p.
- Obstetrics: textbook / ed. V. E. Radzinsky, A. M. Fuks. - M.: GEOTAR-Media, 2021. - 1040 pp.: ill. ISBN 978-5-9704-3376-8
- Code of Practice for Contraceptive Use - a publication of the United Nations Health Foundation and the World Health Organization.
Popular questions
I have inflammation of my left ovary.
The doctor prescribed me several injections and suppositories. Can I replace injections with tablets? I recommend that you consult your doctor regarding this issue to select adequate therapy and change the method of administration.
How to treat an ovarian luteal cyst if I’m pregnant, what should I do?
During pregnancy up to 16 weeks, such cysts require only dynamic monitoring and ultrasound control once a month.
I have a cyst, but I want to get pregnant, please help me.
Hello! Before planning a pregnancy, you need to understand the nature (genesis) of the ovarian cyst and how much it will affect conception and pregnancy. Therefore, you should immediately consult a specialist.
I suspect inflammation and cysts. The doctor prescribed IV thiosulfate, IM ceftriaxone, and Diclovit suppositories. I just didn’t explain, do you need to apply everything at the same time or what?
Hello!
Most often, this complex of treatment is carried out simultaneously, but it is better to check with your doctor. For an accurate diagnosis, contact a specialist
Cystic metastases to the ovaries
Most often, metastases to the ovaries, for example, Krukenberg metastases - screenings of stomach or colon cancer, are soft tissue formations, but often they can also be cystic in nature.
A CT scan reveals cystic formations in both ovaries. You can also notice a narrowing of the rectal lumen caused by a cancerous tumor (blue arrow). Cystic metastases of rectal cancer are clearly visible in the recess of the peritoneum (red arrow), which in general are not a typical finding.
Malignant cystic ovarian tumors
Radiation diagnostic methods, such as ultrasound or MRI, are not intended to determine the histological type of tumor. However, with their help it is possible to differentiate benign and malignant neoplasms with varying degrees of certainty and determine further tactics for patient management. Detection of radiation signs of malignant tumor growth should direct the attending physician (gynecologist, oncologist) to further actively determine the nature of the cyst (surgery with biopsy, laparoscopy). In unclear and contradictory cases, it is useful to re-interpret the MRI of the pelvis, as a result of which you can get a second independent opinion from an experienced radiologist.
Get an MRI of the ovaries in St. Petersburg
Treatment
In 80% of cases they are eliminated on their own: they undergo reverse development. This process takes on average up to 3 menstrual cycles, after which it is necessary to undergo a control ultrasound examination of the uterus and appendages. Large ones are eliminated by laparoscopy. This is one of the few methods that helps get rid of a tumor without extensive dissection of the skin. An additional advantage of the intervention is a rapid postoperative recovery period.
If a follicular cyst provokes ovarian rupture, the woman undergoes emergency surgery: the organ is removed or sutured, depending on the degree of damage. In both cases, after surgery, the patient undergoes hormone replacement therapy.
If the neoplasm appears against the background of oophoritis, in addition to the tumor, it is necessary to eliminate the root cause of its development – inflammation. For this purpose, the woman undergoes antibacterial therapy. When a tumor occurs while taking contraceptives, treatment begins with stopping their use and selecting an alternative type of contraception. If the neoplasm is associated with constant exposure to stress, the woman will need to take sedatives and will additionally need to consult a psychologist.