Gilbert's syndrome is a hereditary disease that is manifested by an increased amount of unconjugated (direct) bilirubin in the blood. This is an autosomal dominant syndrome: the disease occurs if the defective gene is received from at least one of the parents. But even in the presence of a defective gene, clinical manifestations do not always occur. Doctors call this phenomenon incomplete penetrance.
According to various authors, the prevalence of Gilbert's syndrome in Russia is from 5 to 10%. Men get sick 3–4 times more often than women. In 30% of cases the disease is asymptomatic. Only during a biochemical study done for another reason is an increased level of unconjugated bilirubin accidentally discovered.
General information
There are many diseases that are manifested by increased levels of bilirubin - this is a bile pigment (component of bile), which is formed during the breakdown of hemoglobin and myoglobin (proteins containing heme).
Among such diseases can be called Gilbert's syndrome (ICD-10 code E80.4). During the day, the body produces 200-450 mg of bilirubin, which is present in the blood in two forms - indirect (formed in the amount of 250 mg during the daily breakdown of red blood cells) and direct (formed in the liver by binding and excreted in bile). Indirect bilirubin, entering the liver cells, binds to glucuronic acid under the influence of an enzyme. Its combination with glucuronic acid becomes soluble in water, so it easily passes into bile and is excreted in feces, some in urine. Indirect bilirubin is toxic, direct bilirubin is less toxic because it binds to glucuronic acid in the liver (it is also called bound). The key in the process of binding bilirubin is the liver enzyme glucuronyltransferase, with a deficiency of which indirect bilirubin does not bind in the liver and its level in the blood increases (bilirubinemia).
Gilbert's syndrome, what is it in simple words? This is a hereditary disorder of bilirubin metabolism, which is associated with a deficiency or decrease in the activity of glucuronyl transferase. The disease belongs to the class of enzymopathies. A mutation in a certain gene A(TA) 7TAA causes enzyme deficiency and impaired bilirubin uptake, resulting in impaired conjugation of indirect bilirubin and an increase in its level in the blood - benign bilirubinemia due to unconjugated bilirubin. An increase in its level in the blood promotes accumulation in tissues and this explains jaundice. To put it in very simple words, Gilbert's syndrome is a periodically occurring moderate icteric discoloration of the skin, sclera of the eyes and oral mucosa.
Photo showing yellowing of the sclera
Benign (functional) hyperbilirubinemia , which includes Gilbert, Crigler-Nayjar, Rotor, Meulengracht syndrome, are congenital enzymopathies without pronounced changes in the structure of the liver, without signs of hemolysis and cholestasis .
Gilbert's syndrome is characterized by high prevalence - every tenth inhabitant of the globe suffers from it. The ratio of men to women is 3:1. The disease refers to hidden metabolic defects that appear from 3 to 13 years, but mainly in adolescence. The latent form does not manifest itself with any symptoms and is detected by chance during examination. There is a “congenital” version of the syndrome (manifestations develop at 12-30 years of age) and Gilbert’s syndrome, in which clinical manifestations manifest after acute viral hepatitis .
The manifestation of the congenital variant of the disease occurs after physical stress, errors in diet, diseases associated with fever (ARVI, influenza), as well as after mental stress and fasting. The intensity of jaundice in any variant of the disease during an exacerbation is low. In this article we will take a detailed look at Gilbert's disease: what it is, how to treat it, what dangers may be associated with it, and how to prevent exacerbations.
Prognosis for patients
For patients with Gilbert's syndrome, the prognosis is favorable, since if medical recommendations are followed, there are no changes in the liver. The presence of this congenital disease does not affect life expectancy. Deterioration in health occurs when liver disease, hemolytic anemia, or deterioration in the outflow of bile occur.
We recommend reading about how bilirubin changes during hepatitis. From the article you will learn what bilirubin levels will be for different types of hepatitis, and what the dangers of high bilirubin are. And here is more information about how the bilirubin level changes in cirrhosis.
Gilbert's syndrome causes an increase in indirect bilirubin due to a disruption in the activity of the enzyme that converts it into a direct form. It is a genetic disease and most often has a benign course.
Pathogenesis
The process of binding bilirubin in the liver cell is complex and disturbances at any stage affect the development of the disease. The role of the liver in the metabolism of bilirubin is primarily to capture it from the blood by liver cells and deliver it inside the hepatocyte using transport proteins and the enzyme bilitranslocase. Deficiency of this enzyme, which controls the uptake and transport of bilirubin into the liver cell, leads to impaired uptake of bilirubin by hepatocytes and is important in the pathogenesis of the disease. Inside the hepatocyte, bilirubin must be transferred to microsomes, within which it binds to glucuronic acid. Another enzyme is responsible for this transfer - glutathione-S-transferase , the deficiency of which will impair delivery to microsomes.
Finally, the enzyme glucuronyltransferase transports glucuronic acid to bilirubin for binding within microsomes. The deficiency of this main enzyme is associated with mutations in the UGT1A1 gene—in patients, the gene has one extra TA repeat. As a result of such a mutation, enzyme activity decreases by 10-30%. Impaired binding of indirect bilirubin in the liver leads to an increase in its level in the blood - hyperbilirubinemia , the visual manifestation of which is jaundice.
What complications can there be?
The disease is dangerous due to its complications, which arise as a result of the toxic effect of free bilirubin on internal organs. Some scientists do not regard Gilbert's syndrome as a full-fledged disease, calling it a collection of certain symptoms. But this is far from true. This nosological unit has its own characteristics, cause of development and characteristics, which allows us to call it a separate disease.
Hyperbilirubinemia leads to toxic damage to many internal organs, which as a result lose their function. This condition is most dangerous for the structures of the central nervous system. With Gilbert's syndrome, patients often complain of deterioration or loss of memory, impaired physiological reflexes, and mental disorders.
Classification
According to flow options, there are:
- Dyspeptic.
- Asthenovegetative.
- Icteric.
- Latent.
In the dyspeptic variant, the following come to the fore: nausea, possible vomiting, heartburn , pain in the right hypochondrium. The asthenovegetative variant occurs with severe weakness, fatigue, headaches, insomnia , sweating , anxiety , and discomfort in the heart area. With the icteric variant, icteric discoloration of the skin of the face, palms, feet and sclera appears, while the color of urine and feces is not changed. In persons with heterozygous status, a latent form of the disease is observed, which manifests itself only during stress tests (test with fasting, taking phenobarbital , administration of nicotinic acid ).
30% of individuals with the homozygous type of gene carriers have high levels of bilirubin and severe clinical manifestations with jaundice of varying severity. The first episode of jaundice appears after overwork or excessive physical activity, most often at puberty, which is associated with an increase in the level of sex hormones. The disease is characterized by a certain seasonality - from February to July. The surge in exacerbations in February is associated with acute respiratory diseases, and at the beginning of summer - with increased insolation, which causes increased pigment formation. Patients are characterized by a decrease in the detoxification function of the liver.
Why is Gilbert's syndrome dangerous? In general, the disease has a favorable course and is not complicated by liver cirrhosis . Gilbert's syndrome is relatively dangerous, since dysfunction of the biliary system may worsen, chronic cholecystitis , duodenitis and gastroesophageal reflux disease . This syndrome is also dangerous because cholelithiasis may develop. Gilbert's syndrome is often combined with other hereditary diseases (Ehlers-Danlos and Marfan syndrome). These patients have an increased risk of developing adverse reactions when taking certain medications.
In accordance with the schedule of illnesses, which contains health requirements for conscripts, the army is not contraindicated for young men with Gilbert's syndrome, they are not given a deferment, and they are not discharged. However, the soldier needs to organize appropriate conditions: good nutrition and lack of excessive physical activity. But in a military unit it is difficult to fulfill these requirements. These medical prescriptions can be fulfilled while serving as a soldier at headquarters. But people with this disease are denied study at military universities.
An inherited disorder of pigment metabolism is also noted in Crigler-Najjar syndrome , which occurs in two variants. Crigler-Najjar syndrome type I is associated with the absence of glucuronyl transferase in liver cells. It is characterized by intense jaundice, which occurs in the child from the first days of life. The level of indirect bilirubin is 15-50 times higher than normal and there is no direct fraction of bilirubin. Prescribing phenobarbital for this type is ineffective. The disease occurs with bilirubin damage to the brain nuclei and can be fatal. Liver transplantation is the only treatment option.
Crigler-Nayjar syndrome type II is associated with a decrease in enzyme activity, therefore the intensity of jaundice is less than in the previous case and, accordingly, indirect bilirubin is increased no more than 20 times and its direct fraction is determined. An important feature is the good response to treatment with phenobarbital .
The development of bilirubin encephalopathy is very rare. In terms of prognosis, type II disease is more favorable.
Definition of the term
Gilbert's syndrome (Gilbert's disease) is a benign chronic liver disease accompanied by episodic icteric staining of the sclera and skin, and sometimes other symptoms associated with an increase in the concentration of bilirubin in the blood. The disease progresses in waves: periods without pathological signs are replaced by exacerbations, which mainly appear after taking certain foods or alcohol. With constant consumption of food that is “unsuitable” for liver enzymes, a chronic course of the disease may occur.
This pathology is associated with a gene defect transmitted from parents. It does not lead to severe liver destruction, as happens with cirrhosis, but can be complicated by inflammation of the bile ducts or stone formation in the gallbladder (see symptoms of gallbladder diseases).
Some doctors consider Gilbert's syndrome not a disease, but an organismal genetic trait. This is incorrect: the enzyme, the disruption of whose synthesis underlies the pathology, is involved in the neutralization of various toxic substances. That is, if some function of an organ suffers, then the condition can be safely called a disease.
Causes
The cause is a genetic disorder, and provoking factors include:
- Infections, colds.
- Emotional and physical stress.
- Vomit.
- Errors in diet and fasting.
- Drinking alcoholic beverages.
- Drug loads ( ampicillin , chloramphenicol , glucocorticoids, vitamin K , caffeine , paracetamol , rifampicin , anabolic steroids, androgens , salicylates ).
- Various operations.
- Trauma.
- Excessive influence of insolation.
- Premenstrual syndrome.
- Poor sleep, lack of sleep.
Symptoms of Gilbert's syndrome
As we found out, the main symptom of Gilbert's syndrome is yellowness of the skin. The triad of symptoms that was initially described by the author: “liver mask” ( jaundice ), xanthelasma of the eyelids , the frequency of occurrence is distinguished by Gilbert’s disease. Symptoms and treatment depend on bilirubin levels.
As for the yellowness of the skin, it is moderate, has a lemon tint, there is a slight yellowness of the mucous membrane of the mouth, palate and more pronounced yellowness of the sclera. Particular attention is paid to coloring the face, ears, feet, palms, armpits and nasolabial triangle. Jaundice can be constant or intermittent, which is more common and appears when bilirubin rises to 50 µmol/l.
Other symptoms include general weakness, fatigue, sweating , irritability, emotional lability, sleep disturbance. Less common are belching, bitterness in the mouth, bloating, heartburn , nausea, and loss of appetite. Patients become sensitive to cold and often develop goose bumps. When examining a patient, a moderate enlargement of the liver and spleen is sometimes revealed. The latent form does not appear for a long time and can be identified by conducting provocative tests.
These episodes are accompanied by weakness, increased fatigue, emotional lability, dyspepsia (discomfort and unexpressed pain in the right hypochondrium, epigastric region).
It is also possible that there are no complaints and/or visual manifestations of the disease at all. The presence of bile acids in the blood may not be accompanied by jaundice.
Treatment
The question of the need for therapy is decided by the doctor based on the person’s condition, the frequency of remissions, and the level of bilirubin.
Up to 60 µmol/l
Treatment of Gilbert's syndrome, if the unconjugated bilirubin fraction does not exceed 60 µmol/l, there are no signs such as drowsiness, behavioral changes, bleeding gums, nausea or vomiting, but only mild jaundice is noted, drug treatment is not prescribed. Can only be applied:
- phototherapy: illuminating the skin with blue light, which helps water-insoluble indirect bilirubin turn into water-soluble lumirubin and be excreted in the blood;
- diet therapy with the exclusion of the product that provokes the disease, as well as the exclusion of fatty and fried foods;
- sorbents: taking activated carbon, polysorb or other sorbent.
In addition, a person will need to avoid tanning and protect their skin with sunscreen when going out into the sun.
Treatment if above 80 µmol/l
If indirect bilirubin is above 80 µmol/l, the drug Phenobarbital is prescribed at 50–200 mg per day, for a course of 2–3 weeks (it causes drowsiness, so driving and going to work during treatment is prohibited). Preparations with phenobarbital that have a less hypnotic effect can be used: Valocordin, Barboval and Corvalol.
The drug “Zixorin” (“Flumecinol”, “Synclit”) is also recommended: it activates certain liver enzymes, including glucuronyltransferase. It does not cause such a hypnotic effect as phenobarbital, and after its withdrawal it is quickly eliminated from the body.
In addition, other drugs are prescribed:
- sorbents;
- proton pump inhibitors (Omeprazole, Rabeprazole), which will not allow the production of large amounts of hydrochloric acid;
- drugs that normalize intestinal motility: Domperidone (Dormikum, Motilium).
Diet for Gilbert's disease
The diet for the syndrome with hyperbilirubinemia more than 80 µmol/l is more strict. Allowed:
- lean meats and fish;
- low-fat fermented milk drinks and cottage cheese;
- dried bread;
- biscuits;
- non-acidic juices;
- fruit drinks;
- sweet teas;
- fresh, baked, boiled vegetables and fruits.
The consumption of fatty, spicy, canned and smoked foods, baked goods and chocolate is prohibited. You should also not drink alcohol, cocoa or coffee.
Treatment in hospital
If the level of bilirubin is high, or the person has become worse at sleeping, he is bothered by nightmares, nausea, loss of appetite, and hospitalization is necessary. In the hospital, he will be helped to reduce bilirubinemia with the help of:
- intravenous administration of polyionic solutions
- prescription of powerful modern hepatoprotectors
- monitor the correct intake of sorbents
- lactulose preparations will also be prescribed to block the effect of toxic substances that occur during liver damage: Normaze, Duphalac or others.
- importantly, they will be able to administer intravenous albumin or blood transfusions.
In this case, the diet is extremely organic. Animal proteins (meat, offal, eggs, cottage cheese or fish) are removed from it; fresh vegetables, fruits and berries, and fats are excluded. You can only eat porridge, soups without frying, baked apples, biscuits, bananas and low-fat dairy products.
Remission period
During non-exacerbation periods, you need to protect your bile ducts from stagnation of bile in them and the formation of stones. To do this, take choleretic herbs, drugs Gepabene, Ursofalk, Urocholum. Once every 2 weeks, “blind probing” is performed, when xylitol, sorbitol or Carlsbad salt are taken on an empty stomach, then they lie on their right side and warm the gallbladder area with a heating pad with warm water for half an hour.
The period of remission does not require the patient to follow a strict diet, you just need to exclude foods that cause aggravation (this is different for each person). The diet should contain enough fiber-rich vegetables, small amounts of meat and fish, and less sweets, carbonated drinks and fast food. It's best to avoid alcohol completely: even if you don't turn yellow after it, in combination with fatty and heavy snacks, it can lead to hepatitis.
Trying to keep bilirubin at normal levels with an unbalanced diet is also dangerous. It can lead a person to false well-being: this pigment will decrease, but not due to improved liver function, but due to a decrease in the content of red blood cells, and anemia will lead to completely different complications.
Tests and diagnosis of Gilbert's syndrome
How is Gilbert's syndrome diagnosed? If you suspect this disease, there is a certain algorithm:
- Diagnosis of all patients begins with examination and clarification of complaints and causes that provoke the manifestation of jaundice.
- General clinical examinations include a clinical blood test. With this disease, in 30% of cases, patients have high levels of red blood cells and increased hemoglobin (160 g/l or more), in 15% - mild reticulocytosis . An increase in hemoglobin is associated with its excessive synthesis under conditions of increased bilirubin in the blood and tissues.
- Biochemical blood test, including: total bilirubin and its fractions, liver transaminases, total protein, alkaline phosphatase , albumin , cholesterol and triglycerides . These studies diagnose the type of jaundice and the functional state of the liver, including its protein-forming function. The results of studies in patients indicate an increase in total bilirubin (it ranges from 21 to 51 µmol/l and sometimes an increase to 85-130 µmol/l is recorded). An important indicator is an increase in the content of the indirect bilirubin fraction (most often a moderate increase of 18.8-68.4 µmol/l). Liver function tests were unchanged.
- Ultrasound of the abdominal organs - minor changes in the liver are possible.
- Conducting provocative tests.
- The determining factor in diagnosis is a genetic analysis for Gilbert's syndrome, which objectively confirms or excludes the diagnosis. Genetic analysis is based on determining the mutation of the UGT1A1 gene, which encodes the glucuronyl transferase . This gene is located on chromosome 2. Venous blood is taken for analysis and a direct DNA diagnosis of the gene is carried out. A mutation in the promoter region of this gene is manifested by an increase in the number of TA repeats (normally there are 6); if there are 7 or 8 of them on both chromosomes, the functional activity of the enzyme decreases. In homozygous carriers of the mutation, the syndrome occurs with higher levels of bilirubin, severe manifestations, and they are more likely to have cholelithiasis or bile sludge. Heterozygous carriers have a latent form of the disease, but even carriage in this variant requires changes in lifestyle and a more serious attitude towards the choice of medications taken. Homozygous for a trait is a carrier who has the same allelic genes (AA, OO or aa, oo) on both homologous chromosomes. If these alleles are different (AO, ao), this is a heterozygous carrier.
You can get tested for Gilbert's syndrome in many medical laboratories: Hemotest, Invitro, Optimum, DNAcom, CityLab, turnaround time is 10 days. The price of analysis for Gilbert's syndrome varies in different laboratories and ranges from 3300-4610 rubles. You can keep an eye out for promotional offers when the price is halved.
Genetic analysis is important in order to know the possibility of transmitting Gilbert's syndrome to offspring. In the case where both parents suffer from this disease, all their children will also be sick. If one parent is a carrier and the other is healthy, then half the children will be healthy and half will be affected. If one parent is a carrier of the gene and the other is sick, then the child has a 50% chance of having the disease.
What happens in the body with this syndrome
Bilirubin, which causes human skin and eye whites to turn sunny, is a substance formed from hemoglobin. After living for 120 days, the red blood cell, erythrocyte, disintegrates in the spleen, releasing heme, an iron-containing non-protein compound, and globin, a protein. The latter, breaking down into components, is absorbed by the blood. Heme forms fat-soluble indirect bilirubin.
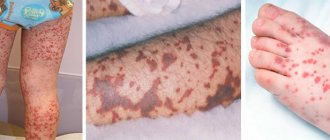
During an exacerbation, the skin becomes more icteric in color. The skin of the whole body, as well as certain areas - feet, palms, nasolabial triangle, armpits - can turn yellow.
Since it is a toxic substrate (mainly for the brain), the body tries to neutralize it as quickly as possible. To do this, it is associated with the main blood protein - albumin, which transports bilirubin (its indirect fraction) to the liver.
There, part of it is waiting for the enzyme UDP-glucuronyltransferase, which, by adding glucuronate to it, makes it water-soluble and less toxic. Such bilirubin (it is already called direct, bound) is excreted with the contents of the intestines and urine.
Gilbert's syndrome is pathognomonic by the following disorder:
- penetration of indirect bilirubin into hepatocytes (liver cells);
- delivering it to those areas where UDP-glucuronyltransferase works;
- binding to glucuronate.
This means that in the blood with Gilbert's syndrome the level of fat-soluble, indirect bilirubin increases. It easily penetrates many cells (the membranes of all cells are represented by a double lipid layer). There he finds mitochondria, makes his way inside them (their shell also mostly consists of lipids) and temporarily disrupts the most important processes for cells taking place in them: tissue respiration, oxidative phosphorylation, protein synthesis and others.
While indirect bilirubin is increased within 60 µmol/l (with a normal range of 1.70 - 8.51 µmol/l), mitochondria of peripheral tissues are affected. If its level is higher, the fat-soluble substance has a chance to penetrate the brain and affect those structures that are responsible for performing various vital processes. The most life-threatening is when the centers responsible for breathing and heart function are soaked with bilirubin. Although the latter is not inherent in this syndrome (here bilirubin occasionally rises to high numbers), but when combined with drug, viral or alcoholic damage, such a picture is possible.
When the syndrome manifested itself quite recently, there were no changes in the liver yet. But when it is observed in a person for a long time, a golden-brown pigment begins to be deposited in her cells. They themselves undergo protein degeneration, and the intercellular matrix begins to undergo scarring.
Hyperbilirubinemia in newborns
The term hyperbilirubinemia refers to any increase in the level of bilirubin in the blood above normal. Taking into account the differences in indicators in newborns who were born at different times, hyperbilirubinemia in full-term newborns is considered when the OB level is more than 256 µmol/l, and in premature ones - more than 171 µmol/l. In newborns, direct and indirect bilirubin ; therefore, two types of hyperbilirubinemia : free (or unconjugated) and associated (synonymous with conjugated).
Hyperbilirubinemia code according to ICD-10 is P59. Any hyperbilirubinemia leads to the development of jaundice, but associated bilirubinemia is a pathological condition. Jaundice syndrome in children occurs under various conditions. Jaundice of the newborn period often requires emergency measures, since indirect bilirubin is a neurotoxic poison, especially in prematurity and in a state of hypoxia. Such children are at risk of central nervous system damage (bilirubin encephalopathy).
There are various types of jaundice in newborns, which are caused by physiological pathological reasons.
Physiological hyperbilirubinemia is a moderate transient (transient) increase in unconjugated bilirubin that occurs in the neonatal period. Hyperbilirubinemia can occur in every newborn, but 50-70% manifest as jaundice (more common in premature and immature newborns).
Physiological jaundice is characterized by:
- Appears after 36 hours of a newborn’s life.
- The peak increase in total bilirubin in a full-term baby occurs on the 3-4th day and on the 5-6th day in a premature baby.
- The child's condition does not suffer: he is active, has a good sucking reflex, normal temperature, there are periods of sleep and wakefulness, the liver and spleen are not enlarged, urine and feces are normally colored.
- A decrease in indicators by the 14th day in a full-term baby and by the 21st day in a premature baby.
Physiological jaundice has no cure, but children should receive exclusive breastfeeding, which helps to overcome jaundice faster. The child should suck often and for as long as he wants, at any time of the day and at least 8-12 times. In the vast majority of cases, jaundice in newborns is physiological, but pathological jaundice must not be missed.
Pathological jaundice has the following features:
- Appears during the first day or is detected on the feet and palms immediately after birth.
- Possible appearance on the 7th day.
- The rate of increase in OB is 85 µmol/l/day.
- The condition of the newborn is unsatisfactory, pathological symptoms are present.
- Enlarged liver and spleen.
- Discolored stool (or dark urine).
- Prolonged jaundice without a tendency to decrease - after the 14th day of life and the 21st day, respectively, in full-term and premature infants.
Pathological hyperbilirubinemia can be caused by various conditions and diseases, including:
- Caused by increased production of bilirubin (these are so-called hemolytic jaundices) in hemolytic disease of the newborn, drug hemolysis , polycythaemic syndrome , ingestion of maternal blood, hemoglobinopathies .
- Arose against the background of polycythemia .
- Developed during infectious diseases.
- Conjugation: hereditary functional bilirubinemia (Gilbert, Arias, Crigler-Nayjar syndromes), metabolic disorders, impaired bilirubin conjugation in intestinal obstruction and pyloric stenosis .
- Caused by drugs or toxins.
- Caused by immaturity of the liver (for example, late onset of conjugation, when the AB count of the indirect fraction increases).
- Mechanical jaundice due to abnormal development of the biliary tract, bile thickening syndrome, familial cholestasis , cystic fibrosis , compression of the biliary tract by various formations.
Among congenital functional bilirubinemias, Gilbert's syndrome ranks first. In newborns, this disease is similar to transient jaundice. The child has hyperbilirubinemia for a long time, but there are no other pathological changes, and there are no cases of kernicterus.
Diagnosis is made based on family history. Prescribing phenobarbital gives good results. The prognosis is favorable. Apparently healthy parents in whom the syndrome is latent may give birth to a child with this syndrome. In this regard, if there have been cases of the disease in the family, the parents need to undergo a genetic examination.
In terms of time of manifestation and severity, the first place is occupied by Crigler-Nayjar syndrome type I. This is congenital familial non-hemolytic jaundice associated with the complete absence of the enzyme glucoronyltransferase , necessary for the conjugation of bilirubin. With this syndrome, liver function is normal, there is no hemolysis and Rh conflict. This syndrome manifests itself in the first days of life with a significant increase in unconjugated bilirubin (up to 400-450 mg/l) and severe kernicterus: muscle hypertonicity , nystagmus , suppression/absence of the sucking reflex, hypotension , convulsions , lethargy .
Clinically, jaundice is noted. Unconjugated bilirubin can reach a concentration of fecal urobilinogen of no more than 100 mg/l. The use of phenobarbital has no effect. The prognosis is very poor, children rarely live beyond 1.5 years.
Crigler-Nayjar syndrome type II proceeds favorably, since the activity of the enzyme glucoronyltransferase is only reduced and liver function is not impaired. The level of unconjugated bilirubin ranges from 60-250 mg/l, especially high in the first months of life, and bilirubin encephalopathy can be observed. There was a positive response to treatment with phenobarbital.
Hemolytic disease of newborns develops when the blood of mother and child is incompatible according to the Rh factor or blood groups. The disease can occur in icteric, edematous and anemic forms. Edema is the most severe and often children are not viable. The icteric form is more favorable, but can also threaten the health of the newborn. In mild cases (indirect bilirubin level less than 60 µmol/l), conservative treatment is carried out. For moderate to severe hemolytic disease, a replacement blood transfusion may be required, and photo and infusion therapy is used before the procedure.
Jaundice in hemolytic disease is either congenital or appears on the first day of life. It has a pale yellow tint, constantly progresses and symptoms of bilirubin intoxication (CNS damage) appear. The liver and spleen are enlarged, the color of feces and urine does not change. Damage to the central nervous system develops when the level of indirect bilirubin is more than 342 µmol/l; for premature and extremely preterm infants this figure is almost 2 times lower. The depth of damage to the central nervous system also depends on the time of exposure of bilirubin to brain tissue.
To prevent hemolytic disease of newborns, women with Rh-negative blood and with group 0(I) are carefully observed, their level of Rh antibodies is determined, and, if necessary, they are delivered early. All women with Rh negative blood are given anti-D globulin . In cases of obstructive jaundice in newborns, various surgical operations are performed to remove obstacles to the outflow of bile.
Factors provoking the development of the syndrome
Today there are a number of factors that are likely to provoke an exacerbation of Gilbert's syndrome or its exacerbation:
- Frequent consumption of fatty foods.
- Alcohol intoxication or regular drinking of alcoholic beverages.
- Long courses of treatment with antibiotics, non-steroidal anti-inflammatory drugs, uncontrolled use of anabolic steroids and the like.
- Treatment with hormonal drugs.
- Strict diets, fasting, refusal to drink water.
- Surgical interventions of varying complexity and localization, medical manipulations.
- Exhausting physical work, intense physical training.
- Stress, psychological disorders.
- Acute infectious diseases.
- Inflammatory processes in the liver.
- Diseases of the digestive tract.
- General hypothermia, overheating of the body, excessive insolation.
- Hormonal imbalance, menstruation.
These factors are not capable of causing a gene mutation. They can only aggravate the clinical situation of an existing disease and provoke its relapse. If you avoid harmful effects on the body in every possible way, then you can live with Gilbert's syndrome all your life and not encounter its clinical manifestations.
Background liver diseases, in particular hepatitis and cirrhosis, can aggravate the course of the disease. In such cases, when the concentration of free bilirubin in the blood reaches 60 µmol/l, the substance penetrates into the cells and affects the mitochondria. Such disorders are manifested by a lack of cellular respiration and lead to energy deficiency.
When the concentration of bilirubin is more than 60 µmol/l, it penetrates into the cells of the head of the central nervous system, affecting the centers of the respiratory and cardiovascular systems. The described disorders are not characteristic of Gilbert's syndrome and are diagnosed only if it is combined with liver diseases.
Gilbert's syndrome and pregnancy
Pregnant women with this disease should be observed by obstetricians-gynecologists, gastroenterologists, and also undergo consultation with a medical geneticist. Women suffering from this disease undergo a molecular diagnostic test that differentiates the heterozygous form of carrier of the gene and homozygous forms of the gene. The risk of a child inheriting the disease will be increased only if the husband carries this gene, so before planning a pregnancy, both parents need to be examined.
During pregnancy, the disease is detected based on clinical symptoms. In most cases, it is benign and during pregnancy there is a decrease in bilirubinemia, which is explained by the induction of the enzyme glucoronyl gransferase by estrogens. Gilbert's disease is not a contraindication to pregnancy and does not have a negative effect on the fetus or pregnancy.
The woman successfully carries the child to term and gives birth. If you follow a dietary regimen, exacerbations are extremely rare and not pronounced. In some women, this syndrome is detected only during the second or third pregnancy, and in previous pregnancies there was no increase in bilirubin. And only some develop itchy skin , yellowing of the sclera, urticaria or atopic dermatitis .
Specific treatment is not carried out during pregnancy (or is carried out in exceptional cases with a significant increase in bilirubin - sorbents, ursodeoxycholic acid ), however, the woman should follow general recommendations:
- physical activity is excluded;
- alcohol;
- strict adherence to a diet with the exception of fatty, fried, smoked foods, canned food, products with dyes and flavor enhancers;
- eating regularly, without skipping;
- It is recommended to avoid stressful situations;
- sufficient sleep;
- limited sun exposure.
Antibiotics increase bilirubin
It is clear that when you weaken the antitoxic function of the liver by using any substance that is not beneficial for it, you increase the risk that the liver cells will not have enough strength to neutralize all toxins.
Therefore, in principle, any medications can increase bilirubin, but it has been noticed that antibiotics are the most effective. This is because the inflammatory response produces many damaged cells, which the body must get rid of over time. But when taking antibiotics, endotoxins from the microbes they kill also enter the bloodstream en masse. In addition, the metabolites of antibiotics themselves are unsafe for the liver cells through which they are excreted. Therefore, the more active and prolonged the antibacterial therapy, the more carefully the liver needs to be protected. In this case, blood purification is prohibited, since Zosterin Ultra will reduce the effect of antibiotics. But Liver 48 can and should be used for a month, directly in parallel with antibiotics. This will give the doctor the opportunity to carry out the course he wants, and you will be able to survive it without compromising your general condition.
In addition, you can simultaneously eliminate the risk of hepatocyte damage from toxins absorbed from the intestines. Antibiotics always cause dysbiosis, which means increased intoxication and load on the liver. Probiotics are now always prescribed along with antibiotics. So use those that really work - Unibacter and also for a month, and not as a decorative weekly course.
More about the program
This way you will prevent the liver from being weakened by antibiotics and therefore the likelihood that bilirubin will not increase due to antibiotics is much higher.
Diet
Diet 5th table
- Efficacy: therapeutic effect after 14 days
- Duration: from 3 months or more
- Cost of products: 1200 - 1350 rubles per week
It has already been said above that the diet of patients should be regular (long breaks between meals and fasting are prohibited), moderate (do not overeat) and dietary. Patients are prescribed Diet No. 5 , excluding fatty and spicy foods, fried foods, cooking fats, canned food, smoked foods, products with cream, coffee, cocoa, and chocolate.
Ways to lower bilirubin
After detecting a high liver pigment coefficient in a blood test, patients are concerned about how to reduce bilirubin.
First of all, it is necessary to establish and exclude the cause that caused the increase in enzyme levels. If this is a concomitant disease, then it must be cured, otherwise jumps in bilirubin levels will recur.
The doctor will select the appropriate complex therapy and prescribe treatment, analyzing the symptoms, medical history and general health of the patient.
In addition to drug treatment, a strict diet will be recommended:
- The basis of the diet should be various porridges and cereal side dishes.
- It is advisable to cook first courses only with vegetable broth.
- More dairy products and sweet fruits.
- The consumption of fresh juices, jelly, compotes, and herbal teas is allowed.
- Use meat and fish products with a low percentage of fat.
- Fractional meals in small portions.
- Exclude citrus fruits, spicy vegetables and spices from the menu.
- Alcohol, soda, strong tea and coffee are also prohibited.
- Smoked, fatty foods, and fried foods will only aggravate the problem.
As auxiliary measures, you can turn to traditional medicine.
Drug treatment
The main goal of drug therapy prescribed by a doctor will be to treat concomitant illness, relieve symptoms and reduce the load on the liver. As a result, drugs such as:
- Hepatoprotectors. Pancreatin and Essentiale will help restore liver cells.
- Choleretic. Allochol normalizes the flow of bile.
- Antibiotics will reduce inflammation.
- Drugs that improve digestion, for example, Mezim.
- Absorbents and antiemetics to relieve symptoms.
- Herbal preparations for cleansing and supporting the liver.
Treatment with folk remedies
To reduce bilirubin, decoctions of medicinal herbs have proven themselves to be effective: mint, oregano, St. John's wort, milk thistle, chicory. The herbs are brewed with boiling water and after infusing for half an hour, they can be taken repeatedly throughout the day.
Effective assistance can be provided by:
- Birch leaves, if you brew them with two glasses of boiled water and drink after 30 minutes of settling for about 7 days at night.
- Drink 100 ml of beet juice twice a day.
- Brew dry motherwort in boiling water for 30 minutes and drink on an empty stomach for 14 days.
- Corn. Infuse dried stigmas in boiling water and drink a quarter glass before meals.
Prevention
Parents who have had a child with this disease should definitely consult and be examined by a geneticist before planning their next pregnancy. This also applies to married couples planning to have children if their relatives are diagnosed with this syndrome.
To prevent exacerbations, it is important for the patient to:
- Compliance with the diet and quality of nutrition.
- Dietary food within table No. 5.
- Moderate physical activity without overload.
- Compliance with the work and rest regime.
- Hardening and a healthy lifestyle.
- Sanitation of chronic foci of infection.
- Treatment of pathology of the biliary tract.
- Rational use of medications. This primarily concerns the intake of glucocorticoids, anabolic steroids, Rifampicin , Streptomycin , Cimetidine , Levomycetin , Ampicillin , caffeine , paracetamol , diacarb .
- Consumption of alcoholic beverages is prohibited.
- Conducting preventive courses of ursodeoxycholic acid for biliary sludge .
Diagnostic measures
Diagnosis begins with studying clinical symptoms and collecting family history. Doctors find out:
- Did the patient’s relatives have liver diseases manifested by jaundice;
- When did the first symptoms of pathology appear?
- How often does the disease worsen and how long does this period last?
- What causes jaundice?
- Presence of concomitant chronic diseases.
During a visual examination, a yellow tint of the skin and sclera is detected, palpation reveals hepatomegaly, and heaviness in the right hypochondrium.
Laboratory diagnosis is important in identifying the disease.
- Hemogram – reticulocytosis, signs of anemia.
- Blood test for biochemical markers of the liver - an increase in the concentration of total bilirubin.
- A medical genetic blood test is carried out by performing a polymerase chain reaction, during which the defective gene responsible for the occurrence of the pathology is identified. The study requires venous blood or buccal epithelium - scraping from the oral mucosa.
- Liver puncture and histological examination of the biopsy sample - to exclude malignant neoplasms, cirrhosis and hepatitis.
There are special tests to make the correct diagnosis. When the antibiotic “Rifampicin” or the vitamin supplement “Nicotinic acid” is introduced into the body, the level of bilirubin in the blood rises sharply. In people who are fasting or limiting their daily caloric intake to 500 kcal, the concentration of bile pigment increases significantly in just a couple of days. The sleeping pill Phenobarbital and its analogues reduce the level of bilirubin in the blood.
A doctor may suspect Gilbert's syndrome based on the following criteria:
- High concentration of total bilirubin in the blood,
- Optimal indicators of liver markers - ALT and AST,
- Normal levels of albumin, alkaline phosphatase and blood coagulation parameters.
Instrumental research methods are used in differential diagnosis when it is necessary to exclude other liver pathologies - neoplasms, cirrhosis, hepatitis, calculous cholecystitis, cholangitis. Patients undergo ultrasound, CT and MRI of the liver. These methods confirm the presence of hepatosis, a disease characterized by metabolic disorders in the liver lobules. The etiology of such processes cannot be established using these techniques.
List of sources
- Diseases of the fetus and newborn, congenital metabolic disorders / ed. R. E. Berman, V. K. Vaughan. M.: Medicine, 1991. 527 p.
- Podymova S. D. Liver diseases. M.: Medicine, 1993. - 544 p.
- Kolyubaeva S.N., Kulagina K.O., Petrova I.S., Krivoruchka A.B., Ivanova A.M. Molecular genetic diagnosis of Gilbert's syndrome using pyrosequencing. Laboratory of health care facilities. 2016; 8:4–6.
- Goncharik I.I. Gilbert's syndrome: pathogenesis and diagnosis / I.I. Goncharik, Yu.S. Kravchenko // Clinical medicine. - 2001. - No. 4. - P. 40-44.
- Kuznetsov A.S., Fomina I.G., Tarzimanova A.I., Oganesyan K.A. Differential diagnosis of benign hyperbilirubinemia // Clinical medicine. - 2001. - No. 3. - P. 8-13.
Alcohol at elevated levels
About algogol - even simpler. The dose matters. Even if you have Gilbert's syndrome, a glass of dry wine is unlikely to hurt. But if the mass dose of ethyl alcohol that you drink is high - strong drinks, then the dose there should, alas, already be 50 ml. Fortified wines, various liqueurs, liqueurs, champagne, beer with preservatives, tequila, etc. absolutely not suitable. But even in this case: if you regularly take care of your liver, then it will not feel any slight disturbance. Read on to learn how to restore the functioning of hepatocytes. It's simple!