Clinic and causes of infection
Streptoderma is a contagious disease, the causative agent of which is transmitted through airborne dust or through direct and household contact with a sick person. For example, dust gets on the wound, or the pathogen is transmitted from an infected person through hands, toys, or common objects, especially if sanitary and hygienic standards are not observed in the family or team.
Streptoderma is caused by beta-hemolytic streptococcus from group A. After infection with the microbe, flaky round spots soon form on a person’s skin, and then purulent patches appear on them. Streptoderma is divided into 2 types: superficial - impetigo and deep - ecthyma. Each has several forms.
First, streptococcus penetrates the skin if the integrity of the skin at the site of contact with the pathogen is damaged. After infection, the incubation period for streptoderma begins, lasting 1 - 1.5 weeks. During this time, the microbe multiplies, but provided that there are predisposing factors for development. For example, unsanitary conditions, a person has a weakened immune system, he has other infectious foci in the body or diseases of a chronic nature: vitamin deficiency, pathologies of the cardiovascular and endocrine systems, etc.
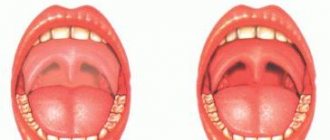
With the end of the incubation period, pink or red spots with jagged edges appear on the skin. In the second stage, the temperature often rises, the skin may peel off, it begins to itch, single or multiple blisters with exudate appear at the site of the lesion, the infection penetrates deeper into the tissue, after which streptoderma goes away with complications. When the purulent element opens, an ulcer forms, and the leaked contents quickly dry out and turn into hard crusts.
Forms of streptoderma:
- tourniol (nail fold infection);
- simple (streptococcal impetigo);
- vesicular;
- erythemo-squamous (dry);
- diaper rash;
- angular stomatitis (jam);
- pityriasis alba;
- vulgar ecthyma.
Examination and treatment should begin as soon as the first signs of infection appear, since inflammation quickly spreads to new areas of the body. After suffering from impetigo, spots without pigmentation are visible on the skin for several months, but ecthyma can leave scars or scars. If therapy is not carried out in a timely manner, recovery occurs no earlier than in a month.
Streptococcus (streptococci)
Streptococci
(lat.
Streptococcus
) is a genus of gram-positive facultative anaerobic bacteria.
Spherical cells with a diameter of less than 2 microns are arranged in pairs or in chains. The vast majority of strains are immobile. Among streptococci there are causative agents of various human diseases, and representatives of normal microflora that live in the oral cavity, gastrointestinal tract, genitourinary and respiratory tract, and strains widely used in the food and pharmaceutical industries. Streptococci are detected in the stomach of 55.5% of healthy people in an amount of 4 lg CFU/g (Zimmerman Ya.S.). Streptococcus spp.
(among them
S. mitis
and
S. parasanguinis
) are the most common bacteria in the microbiota (along with lactobacilli, veillonella and prevotella) in patients with stomach cancer (Starostin B.D.). Streptococci are found in the baby's gastrointestinal tract a few hours after birth. Colonization of the gastrointestinal tract with streptococci occurs during its birth, when the newborn passes through the mother’s birth canal (Khavkin A.I. et al.).
Within the genus, streptococci are classified according to various characteristics, in particular by the type of hemolysis, by serological properties, etc. There is no absolutely unambiguous correspondence between species and serological groups.
Streptococci are associated with bronchial asthma, multiple sclerosis; titers of streptococci decrease in Crohn's disease and increase in colorectal cancer ( Streptococcus bovis
), atrophic gastritis, stomach cancer;
Streptococcus pneumoniae
is associated with adenocarcinoma of the esophagus (Karpeeva Yu.S. et al.).
Classification of streptococci by type of hemolysis
| Pharyngitis caused by streptococcus |
According to the type of erythrocyte lysis determined on blood media, streptococci are divided into the following types:
- α-hemolytic (greening), causing partial hemolysis
- β-hemolytic, causing complete hemolysis
- γ-hemolytic (non-hemolytic), not causing hemolysis
Alpha-hemolytic streptococci
, in particular, include :
- one of the most clinically important pathogens, the causative agent of pneumonia, meningitis and other diseases Streptococcus pneumoniae
- widely used in the preparation of various dairy products, including yogurt, fermented baked milk, varentsy, sour cream, mozzarella and other cheeses, as well as the species Streptococcus thermophilus
- so-called “greening” streptococci: Streptococcus salivarius, Streptococcus mutans, Streptococcus sanguis, Streptococcus mitis
and others.
They are low-virulent and can be part of the normal microflora of the oral cavity, living on the teeth and gums. Some streptococci from this group can cause or contribute to the occurrence of caries (Novikova V.P., Shabalov A.M., Smirnova M.A.), in particular, Streptococcus mutans
. The peculiarity of such streptococci is their transmission from person to person. most often to the child from the mother or other family members. Viridinaceous streptococci are the main cause of infective endocarditis.
| Schematic representation of the cell structure of the beta-hemolytic streptococcus Streptococcus pyogenes, surface and secreted virulence factors (Shpynev K.V. et al.) |
Beta-hemolytic streptococci
according to the classification of R. Lancefield are divided into serogroups A, B ... U in accordance with the structure of carbohydrate C cell wall. Beta-hemolytic streptococci include:
- serogroup A
, or
GAS
: the main representative is the pathogenic streptococcus
Streptococcus pyogenes
, which causes a wide range of invasive and non-invasive human diseases, in particular scarlet fever, phagingitis, tonsillitis;
Some strains of S. dysgalactiae subsp.
equisimilis and
Streptococcus agalactiae anginosus - serogroup B
, or
GBS
:
Streptococcus agalactiae
- streptococcus, found in some individuals as part of the normal intestinal microflora, in 20-30% of healthy women - in the urogenital tract; may cause serious infections in newborns and women in labor - serogroup C
(
GCS
includes mainly streptococci that cause diseases in animals, in particular,
Streptococcus equi
(mystery streptococcus) - the causative agent of acute respiratory disease in horses,
Streptococcus equi subsp.
zooepidemicus - pathogen of mammalian diseases and others - the most important members of serogroup D
(
GDS
) have been reclassified as enterococci
Publications for healthcare professionals addressing the role of streptococci in dental disease
- Novikova V.P., Shabalov AM The condition of the oral cavity in patients with gastroesophageal reflux disease (GERD) // Gastroenterology of St. Petersburg. – 2009. – No. 1. - With. 25–28.
- Smirnova M.A. Patterns of development, principles of complex treatment and prevention of caries of contact surfaces of teeth. Abstract of dissertation. Doctor of Medical Sciences, 14.00.21 - dentistry. TGMA, Tver, 2009.
- Aivazova R.A. Clinical diagnostic criteria and evaluation of the effectiveness of treatment of inflammatory periodontal diseases in patients with acid-dependent pathology of the gastrointestinal tract. Abstract of dissertation. Doctor of Medical Sciences, 01/14/14 – dentistry, 01/14/04 – ext. diseases. MGMSU, Moscow, 2021.
On the website gastroscan.ru in the literature catalog there is a section “Diseases of the oral cavity associated with diseases of the gastrointestinal tract.”
Lactic acid streptococci
A number of steptococci are capable of fermenting dairy products; they are widely used in the dairy and cheese industries, in particular in the preparation of lactic acid products and cheeses. The term “lactic acid streptococci” is very often extended not only to representatives of the genus Streptococcus
, but also to
Lactococcus
, also part of the family of streptococci (lat.
Streptococcaceae
) and the genus
Leuconostoc
from the family
Leuconostocaceae
. When describing lactic acid streptococci, the names of bacteria often differ from those accepted in microbiology.
| Lactic acid Streptococcus thermophilus is used in the preparation of fermented baked milk and other products |
In relation to temperature, lactic acid streptococci are divided into mesophilic and thermophilic. In mesophilic species, the optimal temperature is 25-30 °C. The minimum development temperature for mesophilic lactic acid bacteria is 10 °C. Mesophilic lactic acid streptococci include acid formers: Streptococcus lactis, Lactococcus lactis subsp.
cremoris (formerly called
Streptococcus cremoris
) and aromatic streptococci:
Lactococcus lactis subsp.
lactis (old name
Streptococcus diacetilactis
),
Streptococcus acetoinicus, Streptococcus paracitrovorus
(
Leuconostoc citrovorum
),
Streptococcus citrovorus
(
Leuconostoc citrovorum
). Flavor-forming bacteria release increased amounts of volatile acids (acetic and propionic) and aromatic substances (esters, diacetyl) into dairy products. Mesophilic lactic acid streptococci provide active acid formation and clot formation. Their quantity in the finished product reaches 109 CFU per 1 cm3. These microorganisms are constantly present in kefir grains and kefir, accounting for up to 60% of the total microflora of kefir.
Compared to mesophilic bacteria, thermophilic ones develop better at elevated temperatures (38-45°C, minimum - 20-22°C, maximum - 45-50°C) and ferment sucrose. Thermophilic streptococci include Streptococcus thermophilus
.
Streptococci in the taxonomy of bacteria
According to modern concepts, the genus streptococcus ( Streptococcus
) is included in the family
Streptococcaceae
, order
Lactobacillales
, class
Bacilli
, phylum
Firmicutes
, <group without rank>
Terrabacteria group
, kingdom Bacteria.
In the genus Streptococcus
includes the following species:
S. acidominimus, S. agalactiae, S. alactolyticus, S. anthracis, S. australis, S. azizii, S. B-6, S. bovimastitidis, S. caballi, S. cameli, S. canis, S. caprae, S. castoreus, S. caviae, S. criae, S. criceti, S. cristatus, S. cuniculi, S. danieliae, S. dentapri, S. dentasini, S. dentiloxodontae, S. dentirousetti,, S dentisuis, S. devriesei, S. didelphis, S. downei, S. entericus, S. equinus, S. ferus, S. fryi, S. gallinaceus, S. gallolyticus, S. gordonii, S. halichoeri, S. henryi , S. himalayensis, S. hongkongensis, S. hyointestinalis, S. hyovaginalis, S. ictaluri, S. infantarius, S. infantis, S. iniae, S. lactarius, S. loxodontisalivarius, S. lutetiensis, S. macacae, S Macedonicus, S. marimammalium, S. marmotae, S. massiliensis, S. merionis, S. milleri, S. minor, S. mitis, S. moroccensis, S. mutans, S. oralis, S. oricebi, S. oriloxodontae , S. orisasini, S. orisratti, S. orisuis, S. ovis, S. ovuberis, S. panodentis, S. pantholopis, S. parasanguinis, S. parasuis, S. parauberis, S. pasteuri, S. pasteurianus, S peroris, S. pharyngis, S. phocae, S. pluranimalium, S. plurextorum, S. pneumoniae, S. porci, S. porcinus, S. porcorum, S. pseudopneumoniae, S. pseudoporcinus, S. pyogenes, S. ratti , S. rifensis, S. rubneri, S. ruminantium, S. rupicaprae, S. salivarius, S. saliviloxodontae, S. sanguinis, S. sciuri, S. seminale, S. sinensis, S. sobrinus, S. suis, S tangierensis, S. thermophilus, S. thoraltensis, S. timonensis, S. troglodytae, S. troglodytidis, S. uberis, S. urinalis, S. ursoris, S. varani, S. vestibularis, S. viridans,
as well as groups species:
S. anginosus, S. dysgalactiae
.
To the group Streptococcus anginosus
species included:
S. anginosus, S. constellatus, S. intermedius.
To the group Streptococcus dysgalactiae - S. dysgalactiae
and
S. equi
.
The species Streptococcus equi
has subspecies:
Streptococcus equi subsp.
equi, Streptococcus equi subsp. ruminatorum, Streptococcus equi subsp. zooepidemicus .
Some strains of Streptococcus equi subsp. zooepidemicus
and
Streptococcus equi subsp.
equi are producers of hyaluronic acid and are used as such in the pharmaceutical industry.
Previously, group D streptococci included species that were later transferred to the genus Enterococcus. Specifically, Enterococcus faecalis
was called
Streptococcus faecalis, Enterococcus faecium
was called
Streptococcus faecium
.
Streptococcus lactis species widely used in the dairy and cheese industries
, as well as previously related to streptococci
Streptococcus plantarum, Streptococcus raffinolactis
have been reclassified into
Lactococcus lactis, Lactococcus plantarum
and
Lactococcus raffinolactis
.
Streptococci and diseases caused by streptococci in ICD-10
Streptococci and streptococcal-related diseases are mentioned in the International Classification of Diseases ICD-10 in a significant number of sections, in particular in:
- "Class I. Certain infectious and parasitic diseases (A00-B99)", in blocks:
- “A30-A49 Other bacterial diseases”, in the categories:
- A40 Streptococcal septicemia
- A40.0 Septicemia caused by group A streptococcus
- A40.1 Septicemia due to group B streptococcus
- A40.2 Septicemia due to group D streptococcus
- A40.3 Septicemia caused by Streptococcus pneumoniae
. Pneumococcal septicemia - A40.8 Other streptococcal septicemias
- A40.9 Streptococcal septicemia, unspecified
- A49.1 Streptococcal infection, unspecified
- B95.0 Group A streptococci as a cause of diseases classified elsewhere
- B95.1 Group B Streptococcus as a cause of diseases classified elsewhere
- B95.2 Group D streptococci as a cause of diseases classified elsewhere
- B95.3 Streptococcus pneumoniae
as a cause of diseases classified elsewhere - B95.4 Other streptococci as a cause of diseases classified elsewhere
- B95.5 Unspecified streptococci as a cause of diseases classified elsewhere
- “J10-J18 Flu and pneumonia”, in the categories:
- J15.3 Pneumonia due to group B streptococcus
- J15.4 Pneumonia caused by other streptococci
- “P35-P39 Infectious diseases specific to the perinatal period”, in the headings:
- P36.0 Neonatal sepsis due to group B streptococcus
- P36.1 Sepsis of the newborn due to other and unspecified streptococci
- P36.2 Sepsis of the newborn due to
Staphylococcus aureus - P36.3 Sepsis of the newborn due to other and unspecified staphylococci
Back to section
Diagnosis of streptoderma
There are many skin diseases that manifest themselves as rashes or spots or other signs characteristic of streptococcal infection: atopic dermatitis, herpes zoster, microbial eczema, chickenpox, ulcerative-vegetative pyoderma, and so on. Therefore, during the examination, the doctor carries out differential diagnostics and takes biomaterial from the surface of the damage for laboratory research.
If streptoderma is suspected, the following tests are performed:
- bacteriological (discharge from wounds, blisters);
- blood (general, sugar, sterility, hormonal status, immunogram, HIV, syphilis);
- feces for the presence of helminths;
- urine general.
Bacteriological examination of biomaterial helps to identify infectious agents and their susceptibility to drugs. The results of a general blood test in the chronic form of streptoderma sometimes show no deviations from the norm, but more often an increase in neutrophils (a type of leukocyte) and an increase in the erythrocyte sedimentation rate are determined, which indicates an inflammatory process in the body.
To conduct research for immunodeficiency and sexually transmitted diseases, the patient's consent is required. In case of complications or detected pathologies accompanying streptoderma, the blood is analyzed for sterility, hormone levels, and an immunogram is performed.
The role of laboratory tests is important to establish the types of pathogenic microorganisms that caused the infection. After all, streptococcus often joins if there is already a disease that damages the skin, for example, dermatitis, eczema, herpes, and so on. During the examination, doctors look for the main cause of the infection, determine the form of streptoderma, and select the optimal treatment. The right combination of medications speeds up the healing process.
Streptococcus pyogenes, DNA [real-time PCR]
A study to identify the causative agent of streptococcal infection (Streptococcus pyogenes), during which the genetic material (DNA) of streptococcus in a sample of biomaterial is determined using the real-time polymerase chain reaction method.
Synonyms Russian
Streptococcus pyogenes, group A beta-hemolytic streptococcus, GABHS, group A beta-hemolytic streptococcus, β-HSA [real-time polymerase chain reaction, real-time PCR].
English synonyms
S. pyogenes, Group A streptococcus, GAS, β-hemolytic streptococcus group A, β-hemolytic streptococcus group A.
Research method
Real-time polymerase chain reaction.
What biomaterial can be used for research?
A swab from the pharynx (oropharynx), a swab from the nasopharynx, a urogenital scraping.
General information about the study
S. pyogenes is a Gram-positive, spherical bacterium that is the causative agent of acute pharyngitis and impetigo, as well as a spectrum of more severe destructive diseases such as pneumonia, sepsis and septic arthritis, toxic shock syndrome, cellulitis and necrotizing fasciitis.
Traditionally, to confirm the diagnosis of streptococcal infection, bacteriological seeding of biomaterial on special media is used. The biomaterial can be discharge from the tonsils or nasopharynx (if acute pharyngitis is suspected), or sputum (for pneumonia). As a rule, the result can be obtained only after a few days, which is associated with a delay in making an accurate diagnosis and prescribing specific treatment. However, it has been revealed that timely diagnosis and specific treatment not only reduce the duration of the disease and the intensity of symptoms, but also reduce the risk of developing complications such as peritonsillar abscess, otitis media, acute rheumatic fever and post-streptococcal glomerulonephritis (for acute pharyngitis), streptococcal sepsis (for pneumonia ), joint destruction and disability (with septic arthritis). Empiric therapy with penicillin antibiotics is based on the premise that S. pyogenes is the main bacterial causative agent of acute pharyngitis (5-15% of cases in adults and 20-30% in children). It should be noted that acute pharyngitis can be caused by other bacterial or viral agents, for which the appointment of such empirical therapy is not only not justified, but is also dangerous due to the development of resistant strains of microorganisms. Such diagnostic difficulties can be overcome using RT-PCR - polymerase chain reaction - this method allows you to get an accurate result in a shorter time.
The RT-PCR reaction uses specific primers for the S. pyogenes DNA fragment. This feature makes it possible to identify only pyogenic streptococcus, and not other streptococci related to it - representatives of the normal microflora of the pharynx (Streptococcus mutans, Streptococcus viridians). In terms of specificity, RT-PCR is not inferior to bacteriological culture and is significantly superior to other methods of identifying the pathogen (for example, a rapid test for determining the antigen).
Quite often, biomaterial is taken for research during the treatment of the disease. As a result, the sensitivity of diagnostic methods decreases and the likelihood of obtaining a false negative result is higher. In such a situation, the RT-PCR method has some advantages over other types of diagnostics. This is explained by the fact that to identify the pathogen in the reaction, the genetic material of the pathogen is used - both the genomic DNA of a living microorganism and DNA fragments of a bacterium that has undergone lysis. In this case, it becomes possible to identify not only living, actively reproducing microorganisms, but also bacteria killed as a result of treatment. Unlike RT-PCR, a prerequisite for other diagnostic methods (enzyme-linked immunosorbent assay or bacteriological culture) is the presence of living microorganisms. Therefore, if the biomaterial is given during treatment, the RT-PCR method should be preferred to other diagnostic methods.
The high sensitivity of RT-PCR allows this method to be used in the diagnosis of complications of acute pharyngitis: acute rheumatic fever and post-streptococcal glomerulonephritis. Complications of acute pharyngitis are autoimmune diseases in which S. pyogenes - associated pharyngitis is a causative factor in the pathological immune response, but at the time of diagnosis of these complications it has already resolved (on its own or as a result of treatment). Therefore, it is possible to identify the pathogen through bacteriological culture of tonsil and nasopharynx discharge in patients with complications of acute pharyngitis only in a small percentage of cases. On the other hand, proof of previous S. pyogenes infection is a necessary criterion for diagnosis, and also greatly facilitates the differential diagnosis of diseases. The RT-PCR method is characterized by high sensitivity and therefore can be used in the diagnosis of complications of acute pharyngitis.
The detection of S. pyogenes in so-called sterile environments is always a pathological sign. On the other hand, the detection of this microorganism in non-sterile environments (sputum, nasopharyngeal discharge) does not always indicate the presence of a disease. It was found that about 12-20% of school-age children and 2.4-3.7% of adults are asymptomatic carriers of S. pyogenes. In such cases, the interpretation of a positive test result should be assessed taking into account the bacterial load and in combination with some other clinical and laboratory signs. Typically, asymptomatic carriage is characterized by fewer bacteria compared to active infection. Therefore, the finding of a high bacterial load of S. pyogenes in a throat swab from a patient with fever, sore throat, and painful regional lymphadenitis confirms the diagnosis of acute streptococcal pharyngitis. And, conversely, the detection of a low bacterial load of this microorganism in a throat smear in the absence of complaints and clinical picture should be regarded as asymptomatic carriage. RT-PCR is a semi-quantitative method that allows an indirect assessment of bacterial load. Therefore, it turns out to be especially useful when examining “healthy carriers” of streptococcus. Asymptomatic carriage of S. pyogenes should be suspected in a patient when streptococcus is detected after an adequate course of antibiotic therapy, as well as in family members of a patient with frequent exacerbations of streptococcal pharyngitis.
What is the research used for?
For diagnostics:
- acute pharyngitis;
- acute rheumatic fever and post-streptococcal pharyngitis in patients with or without a history of an episode of acute pharyngitis;
- asymptomatic carriage of S. pyogenes in a patient with frequent relapses of pharyngitis;
- asymptomatic carriage of S. pyogenes in family members of a patient with frequent relapses of streptococcal pharyngitis;
- community-acquired pneumonia;
- septic arthritis.
When is the study scheduled?
- For symptoms of acute pharyngitis: pain when swallowing, swelling and erythema of the pharynx mucosa, purulent discharge from the surface of the tonsils, painful regional lymphadenitis;
- for symptoms of acute rheumatic fever: migratory polyarthritis or arthralgia, a feeling of interruptions in the heart, pain in the heart, unmotivated weakness, ring-shaped erythema and subcutaneous nodules, as well as neurological symptoms in the form of choreic hyperkinesis;
- for symptoms of post-streptococcal glomerulonephritis: edema (periorbital or generalized), gross hematuria, unmotivated weakness, proteinuria less than 3.5 g/day, arterial hypertension;
- when examining a patient with recurrent pharyngitis;
- when examining family members of a patient with recurrent pharyngitis;
- when examining family members of a patient with frequent relapses of acute streptococcal pharyngitis;
- in the presence of a risk factor for S. pyogenes (associated pneumonia) such as the H1N1 influenza virus;
- with symptoms of community-acquired pneumonia: sudden onset of illness, fever, shortness of breath, chest pain, cough with purulent sputum;
- in the presence of risk factors for septic arthritis: infancy and old age, immunosuppressive therapy, somatic diseases, hemodialysis;
- for symptoms of septic arthritis: pain in the joint at rest and with movement, erythema of the skin over the joint area, impaired mobility in the joint, increased body temperature and unmotivated weakness.
What do the results mean?
Reference values: negative.
Reasons for a positive result
In the discharge of the nasopharynx and tonsils:
- acute pharyngitis;
- acute rheumatic fever;
- poststreptococcal glomerulonephritis.
In sputum:
- pneumonia;
- acute bronchitis, smoker's bronchitis.
What can influence the result?
- The use of penicillin antibacterial drugs (amoxiclav, ampicillin), cephalosporins (cefixime, ceftibuten) and macrolides (azithromycin, clarithromycin) before taking the material for analysis can lead to a negative result.
Important Notes
- About 12-20% of school-age children and 2.4-3.7% of adults are asymptomatic carriers of S. pyogenes.
- The test result should be evaluated in conjunction with certain other laboratory tests.
Also recommended
- Complete blood count (without leukocyte formula and ESR)
- General sputum analysis
- Antistreptolysin O
- C-reactive protein, quantitative (highly sensitive method)
- Streptococcus pneumoniae, DNA [real-time PCR]
Who orders the study?
General practitioner, ENT, infectious disease specialist, pulmonologist, epidemiologist, traumatologist.
Literature
- Lee JH, Uhl JR, Cockerill FR 3rd, Weaver AL, Orvidas LJ. Real-time PCR vs standard culture detection of group A beta-hemolytic streptococci at various anatomic sites in tonsillectomy patients. Arch Otolaryngol Head Neck Surg. 2008 Nov;134(11):1177-81.
- Uhl JR et al. Comparison of LightCycler PCR, rapid antigen immunoassay, and culture for detection of group Astreptococci from throat swabs. J Clin Microbiol. 2003 Jan;41(1):242-9.
- Chiappini E, Regoli M, Bonsignori F, Sollai S, Parretti A, Galli L, de Martino M. Analysis of different recommendations from international guidelines for the management of acute pharyngitis in adults and children. Clin Ther. 2011 Jan;33(1):48-58.
- Hill HR. Group A streptococcal carrier versus acute infection: the continuing dilemma. Clin Infect Dis. 2010 Feb 15;50(4):491-2.
- García-Arias M, Balsa A, Mola EM. Best Pract Res Clin Rheumatol. Septic arthritis. 2011 Jun;25(3):407-21.
Therapy for streptoderma
Medicines are prescribed according to the patient’s age category and his individual physiological state. The sooner a person turns to doctors, the faster cell regeneration occurs and the sooner the effect of the drug comes.
Treatment of streptoderma with conservative methods is as follows:
- treating wounds with disinfectants;
- applying ointment or gel to the damage;
- injections;
- physiotherapy UFOK, UFO (ultraviolet irradiation of blood, affected skin);
- vitamin therapy;
- taking antihistamines and immunomodulatory drugs;
- diet.
To speed up treatment, the patient must follow medical recommendations and strict sanitary conditions: careful hygiene, sterility of instruments and hands when treating wounds, disinfection of personal belongings.
Antiseptics for streptoderma
To stop the spread of bacteria and dry the wounds, alcohol and water disinfectant solutions are used to treat the skin in case of streptococcal infection. The type of product is selected depending on the location of the damage on the skin.
Chlorhexidine, peroxide, Methylene blue, Miramistin, potassium permanganate and other aqueous solutions are used to treat the area around the eyes, lips, and mucous membranes. These drugs are also used to treat streptoderma in infants, children, people with sensitive skin, or if allergic dermatitis is confirmed, to which an infection is associated.
Alcohol solutions: green, blue, iodine, Fukortsin, Boric or Salicylic acid cannot be used to treat wet wounds, mucous membranes, lips, eyelids, skin if you are individually intolerant to the drug. They are prohibited if there are age or other contraindications for use.
Before treating skin with streptoderma, you should disinfect your hands. All actions are carried out using sterile cotton or gauze swabs. If bubbles with pus (bullas, phlyctenas) have formed in the area of damage, they are punctured, then the antiseptic is reapplied. During the treatment, the rash also includes healthy skin approximately 1 cm around the rash. The procedure is repeated up to 4 times a day, and half an hour after the manipulation is completed, local therapy is used.
Other medications in the treatment of streptoderma
After treating erosions, you must use ointments, gels or pastes that contain antimicrobial and antiseptic substances. Local therapy is continued until the wounds are completely healed. For streptoderma, the drugs are applied to the dry surface of the lesions, cleaned with water or alcohol solutions. If the doctor has prescribed the use of drugs in the form of a compress, the procedure is carried out twice a day: the wound is thickly smeared with the product, covered with a gauze cloth, secured with a bandage or adhesive tape and left for 30-60 minutes, according to the instructions in the instructions.
For streptoderma, medications such as Resorcinol, Tsindol,
It is also useful to treat damaged skin with ointments containing an antibiotic: Erythromycin, Tetracycline, Gentamicin, Levomekol, Streptocide, Syntomycin.
For streptoderma, the doctor prescribes the intake of B vitamins (riboflavin, thiamine, folic acid, pyridoxine, cobalamin), as well as A, C, D, E, K, PP, H. They improve cell regeneration, cleanse the body of microbial waste products, and normalize metabolism.
Sometimes treatment is carried out using glucocorticosteroids - drugs containing hormones. The doctor prescribes Pimafucort, Celestoderm B, Lorinden C and other ointments if the patient has streptoderma combined with eczema, atopic dermatitis, ulcers, and allergies to antiseptics.
For ecthyma, multiple skin lesions due to infection, weakened immunity, complications, the doctor prescribes Ospamox, Amoxicillin, Bactoclav, Fromilid, Azitsin and other antibiotics. When using this type of medication, the patient must simultaneously drink probiotics to normalize the intestinal microflora.
To prevent the spread of streptoderma to new areas of the body, it is not recommended to bathe or comb wounds. It is allowed to wipe the skin with chamomile infusion, and apply wet lotions soaked in herbal or oak bark infusions to the rashes to reduce itching and inflammation. For prevention purposes, insect bites, scratches and wounds must be treated promptly with an antiseptic, as well as personal hygiene.