Adhesions are strands of connective tissue that connect adjacent organs in the pelvis. The prevalence of the pathology is extremely high - up to 1-2% of the population, while the deviation in men is 2.7 times less common than in women. After surgical interventions, adhesions form in 16% of cases, during repeated operations - in 95%.
What are adhesions in gynecology
Adhesions occur in the pelvis as a protective reaction of the body to inflammation. At the initial stage, the affected organ swells, and protein films of fibrin may form on its surface.
This occurs already on the third day of the active course of the pathology. At first, fibrin deposits have a soft consistency, but over time, an extracellular (extracellular) matrix is deposited in them:
- collagen;
- glycoproteins;
- hyaluronic acid;
- proteoglycans.
These inclusions make the resulting strands strong and rough. Films can hold both organs together and hollow organs inside.
Ovarian adhesions often occur; the pathology affects both the cervix and its cavity itself. For example, with inflammation of the endometrium, it is precisely such strands that cause “gluing” and lead to significant problems.
When organs are occluded, they become less mobile and mobility is limited. If you seek medical help in time, the adhesive process can be prevented.
You should be especially careful about the problem if there is a threat of Asherman's syndrome - in this case, peritoneal adhesions will form in the area of the cervical canal and the lower part of the uterus.
The presence of synechiae in women threatens with abnormal menstruation, remnants of unresolved mucous membranes and a severe inflammatory process.
With Asherman's syndrome, doctors sometimes diagnosed up to two-thirds of the area of the uterus with involvement of the fallopian tubes in the pathological process.
Pregnancy with such a pathology is impossible, and treatment of extensive adhesions in the pelvis does not guarantee a positive result.
Gynecology has disappointing statistics regarding the presence of adhesions in women.
It has been proven that any surgical intervention or inflammatory process of the organs of the female reproductive system can provoke pelvic adhesions, but the numbers are truly shocking - after gynecological operations, every second patient experiences synechiae, and infections on average cause 75-80 percent of complications in the form of adhesions.
The emerging strands do not always give clear symptoms, so many visits to the clinic occur in severe cases, when the connective tissue can only be removed surgically.
During pregnancy
The question of pregnancy with synechia always worries patients who have been diagnosed with this.
Indeed, problems can begin at an early stage. If there are adhesions in the tubes and pregnancy is planned, then they can cause infertility.
At the same time, practice shows that it is quite possible to become pregnant with synechiae, because a lot depends on the number of adhesions and their quality.
With a small number of elastic, recent formations, conceiving a child is not excluded, and women bear and give birth to healthy children. Therefore, synechiae is not a death sentence; you can get pregnant with them, but it is better to treat them in a timely manner.
With minor adhesions that do not cause symptoms, the woman may not know about them until conception occurs. And only the first examinations by a doctor allow a diagnosis of synechia to be made.
Their presence does not at all make bearing a fetus impossible, however, the pathology can be treated all this time only with limited methods, and most doctors simply monitor the patient, deciding the issue of treatment after childbirth.
During pregnancy, experts advise a woman to adjust her diet, switch to split meals five times a day and give up those foods that cause flatulence.
The presence of adhesions can complicate pregnancy with abdominal tenderness, which is associated with the growth of the uterus. In addition, there is a risk of resumption of the inflammatory process.
While carrying a baby, women can relieve pain with analgesics approved for pregnant women, and non-steroidal anti-inflammatory drugs are used to prevent suppurative processes.
To improve muscle elasticity, special gymnastic exercises are recommended, which a physical therapy doctor will introduce the expectant mother to.
If the cords cannot be eliminated, laparoscopic sparing intervention is performed. The doctor will make the choice of treatment method after a thorough examination of the patient.
Education mechanism
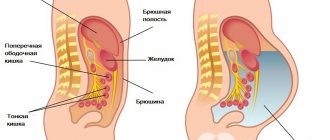
The abdominal cavity is lined from the inside by the peritoneum, a serous membrane that forms a closed space where the abdominal organs are located. The peritoneum is represented by 2 layers: parietal, lining the abdominal cavity, and visceral, enveloping the internal organs. Both layers of the peritoneum are connected to each other and pass into one another. The main functions of the peritoneum are to create mobility of organs, prevent their friction against each other, protect against microbial agents and limit the infectious process when microorganisms penetrate into the abdominal or pelvic cavity.
A damaging factor (trauma or inflammation of the peritoneum) causes the release of mediators that stimulate regeneration. At the initial stage of the process, fibroblasts are activated, producing fibrin. The resulting fibrin fibers cause adhesion of nearby organs and tissues. As a result, the inflammatory focus is demarcated from healthy tissue. If there is extensive traumatic injury or chronic inflammation, the dissolution of connective tissue is disrupted, blood vessels and nerve endings form in the adhesions, and the density of collagen fibers increases. Loose adhesions and layers of the peritoneum become denser, the mobility of the pelvic organs is limited. Any displacement of organs (turning, bending, physical activity) leads to tension in the adhesions, irritation of the nerve plexuses and the appearance of pain in the lower abdomen.
How to treat adhesions
Adhesions in the pelvis can be treated in several ways. Therapy depends, first of all, on the severity of the disease. Conservative treatment of adhesions will be effective as a preventive measure, as well as at the initial stage of treatment of the disease.
The pain in this pathology is not intense, is not constant, and the adhesions themselves are often discovered by chance.
Chronic adhesions in the pelvis are best treated with physiotherapeutic techniques that make the connective tissue softer, thinner and more elastic.
At the initial stage, such therapy helps reduce pain in the abdomen and lower back. And persistent physiotherapy allows you to get rid of synechiae in several courses.
If the adhesions are old and not completely eliminated, adhesions in the pelvis will have to be treated surgically.
In case of adhesions of the fallopian tubes, treatment involves a preliminary diagnosis of the condition of the female genital organs. The decision to undergo laparoscopic surgery is made after diagnosing the fact of tubal fusion.
If patency in the pipes is preserved, treatment begins with physiotherapeutic techniques. In most cases, with uncomplicated pathology, it is possible to do without surgical intervention.
Drug treatment
When treating synechiae, the origin of the pathology and the course of the disease, the severity of the signs of the pathology are taken into account. In the absence of obvious symptoms, the adhesive process must be treated with the most gentle methods possible.
Therefore, at this stage of the disease, tablets will play a major role as the basis for drug treatment of pathology.
Among the drugs used to eliminate adhesions, anti-inflammatory medications are used that can affect the mechanisms of adhesions. Sensitivity is determined by examination of a vaginal smear.
An effective remedy against many representatives of pathogenic microflora is Vilprafen.
This drug belongs to the group of macrolides and contains the active ingredient josamycin. Used in the form of vaginal suppositories.
Another active drug that is often included in the treatment regimen for adhesions is Flamax.
The drug belongs to the anti-inflammatory group; it can act actively in cases of severe pain, since it quickly resolves adhesions and reduces swelling in the affected area. Used in the form of vaginal suppositories.
Longidaza has recently been considered the gold standard in therapy. This medication is used in the second stage of treatment, when the inflammatory process in the patient’s body has already been eliminated.
Longidase has a targeted effect and is active against connective tissue, since it breaks down glycopeptide bonds and promotes the resorption of synechiae.
Form of use: intramuscular injections. Therapy can be carried out in several courses if one is not enough.
Proteolytic drugs that promote fibrin resorption include Trypsin. This drug is successfully used as a component of combination therapy. The release form of the drug is ampoules for intramuscular injection.
An integral means of treatment is the drug Acilact, a representative of probiotics, prescribed at the stage of final therapy of the adhesive process.
With the help of Acylact, you can quickly normalize the vaginal microflora, which suffers significantly during the treatment of synechiae.
The medications listed above are key tools that help eliminate organ adhesions.
When drawing up a treatment regimen taking into account the individual characteristics of the patient, the doctor may replace medications or add combinations of other medications.
Surgical intervention
Surgical treatment for synechiae is carried out to eliminate the painful painful symptoms of the disease, as well as to restore normal mobility of organs.
For large areas of adhesions, doctors use traditional wide access to the pathology, as a result of which the cords are cut with a scalpel.
Surgery is performed urgently or planned. Signs of the need for urgent intervention are the appearance of nausea and vomiting, cramping pain in the lower abdomen, symptoms of intestinal obstruction (flatulence, lack of bowel movements, difficulty evacuating gases from the intestines).
If adhesions in the uterus provoke infertility and do not show signs of acute pathology, then treatment is carried out as planned. Perhaps a more gentle intervention is laparoscopy.
Laparoscopy
Laparoscopic operations are performed using three punctures in the abdominal cavity. Gases are injected into the abdominal cavity to clear the surgical field for the doctor.
Removal of adhesions takes place under video control - the doctor looks at the monitor and operates with miniature instruments, eliminating adhesions one by one.
Laparoscopic intervention significantly reduces the rehabilitation period for patients, and the risk of new strands as complications of laparoscopy is minimal.
Conservative methods
Adhesions in the uterus can be treated conservatively only at the initial stage of their appearance, when the connective tissue cords are not yet so hardened.
As conservative methods, primarily medications are used that directly oppose the development of the inflammatory process.
These can be vaginal suppositories and tablets, and injections are also used.
Gynecological adhesions are well resolved by the drugs Lidaza and Longidaza, which today are actively used in the conservative treatment of the disease.
Therapy with such drugs is carried out in courses, and doctors need to monitor the dynamics of the pathology - if synechiae does not decrease, then they move on to radical methods of helping patients.
If at the initial stage the treatment regimen was drawn up correctly and gave the expected effect, it is possible to treat adhesions in the fallopian tubes without surgery.
This is the most optimal method of treating pathology, but, unfortunately, it is not suitable for all patients.
Physiotherapy
Physiotherapy is extremely important, since only physiotherapeutic techniques can cure minor pelvic adhesions that have just begun to appear in a woman.
The most common method of physiotherapeutic treatment of pathology is electrophoresis with lidase, chymotrypsin and trypsin.
These components are able to penetrate deep into synechiae and provoke the destruction of stable connections between the elements of fibrous cords.
Folk remedies
It is possible to treat adhesions in the fallopian tubes and in other locations with folk remedies only at the first stage of development of the pathology, when the pathological process has not yet become widespread in the organs.
Populists recommend using infusions of medicinal herbs for adhesions, which do absolutely no harm in treating the disease.
The power of herbs allows you to activate blood circulation and lymph flow, which normalizes the synthesis of connective tissue and prevents its uncontrolled growth.
Experts in folk medicine advise actively using flax for adhesions, which has pronounced anti-inflammatory effects. A small amount of flax seeds must be boiled in water to form a thick, slimy liquid.
The broth is filtered, allowed to cool and used as tampons in the vagina. The minimum course of therapy is ten days.
Another effective remedy for synechiae is St. John's wort, which helps activate lymph flow.
To prepare the product, you need to pour five tablespoons of dry St. John's wort into a liter of boiling water and leave for three hours.
As soon as the medicinal liquid has cooled, you can douche with it at night. Such procedures are carried out every evening for three weeks.
Compresses made from medicinal herbs also have a good effect.
To prepare a compress, you need to mix morinda and yarrow in equal proportions and blot a cotton cloth or several layers of gauze with this liquid.
A compress is placed on the abdomen and insulated with a woolen scarf. The compress should be kept for as long as possible; the course of therapy includes ten procedures.
Folk remedies can be treated in combination with medications - this will enhance the effect of the latter and will contribute to the active recovery of the patient.
Popular questions
Good afternoon!
5 years ago there was an operation: the tubes and 1 ovary were removed. Now I am 43 years old and menopause has begun: all the symptoms and menstruation have stopped. Please tell me, is there any treatment option other than hormones? It's a very difficult situation right now. What natural remedies can be used? Thank you Hello! You can use products containing phytoestrogens, antioxidants, and vitamin complexes. This will help alleviate the condition. Such drugs in the line of products include Gynocomfort climafemin. The product is used 1 t once a day for 3 months.
Is it possible to restore tubes if they are cut and tied. If yes, how to do it?
Hello! After sterilization, it is virtually impossible to restore the patency of the fallopian tubes and successful functioning for the implementation of reproductive plans. I recommend contacting a fertility specialist for a possible decision in favor of IVF.
13 years ago I had an ectopic pregnancy, one tube was removed, the second was tied. Is it possible to restore the tube, if not, is IVF done?
Hello! In this case, you should consult a reproductologist to prepare for an IVF program with the indication of tubal factor infertility.
Good afternoon, I had an ectopic pregnancy. On 06/30/19 they had an operation and removed the right tube, but there was no period, although it was supposed to come on 07/22/25. I checked, the test showed 2 stripes, tell me, am I pregnant again?
Hello!
After the operation, there should have been bloody discharge from the genital tract immediately, since the pregnancy was removed and the mucous membrane was rejected from the uterine cavity. Therefore, the cycle will be restored to a new rhythm in 28-32 days. You should have been warned about sexual rest until your cycle returns and the need for contraception for 6 to 12 months. If you did not follow this, then you may be pregnant. The test gives a false positive result up to 1 month after a terminated pregnancy. It is more effective to get tested for hCG levels at intervals of 2 days; a drop should be noted. If, on the contrary, there is an increase, then you should immediately consult a doctor. For an accurate diagnosis, contact a specialist
How to treat adhesions after surgery
Adhesions in the uterus and other organs of the female reproductive system are provoked not only by inflammatory pathologies, but also by surgical interventions.
Postoperative adhesions are a kind of complications after surgery that must be eliminated during the rehabilitation period or immediately after it.
The reasons for the formation of adhesions after surgery are easy to establish - this is the body’s protective reaction to the intervention, so the appearance of adhesions after surgery can be predicted. Treatment of the adhesive process will directly depend on the patient’s health condition.
If the woman’s condition is satisfactory after surgery, anti-adhesion tablets, which have an anti-inflammatory effect, are additionally prescribed.
Enzymatic agents, antibiotics, and other drugs that promote fibrin resorption are recommended. Doctors emphasize movement almost immediately after surgery, as soon as the patient is allowed to stand.
Vigorous activity will prevent adhesions from forming between organs.
When treating postoperative adhesions in the pelvis, physiotherapeutic techniques are used if the state of health and the nature of the intervention allow this.
If a soft fusion forms, then it can be removed conservatively. Usually doctors pay special attention to prevention and do not miss the initial moment of the onset of pathology.
The resulting adhesions, which are not diagnosed in time, become old and are removed surgically.
How to treat adhesions in the fallopian tubes
To treat adhesions in the fallopian tubes, conservative treatment is usually used at an early stage, but if surgery is chosen, doctors tend to use laparoscopic intervention.
Adhesions in the uterus usually occur due to endometriosis, so it is very important after surgery to eliminate any inflammation that could re-provoke the appearance of adhesions.
Adhesions in the fallopian tubes are often a complication of uterine fusion, so they occur both together with this pathology and separately.
Treatment of such adhesions should begin as soon as possible if complete occlusion is observed and the woman is still planning a pregnancy.
Stages of pathology development
At the first stage, adhesions are located near the appendages, without interfering with the movement of the egg and its capture by sperm. The villi of the fallopian tubes are not affected and are able to deliver a fertilized egg to the uterus.
The second stage is characterized by the absence of contact between the egg and sperm, as a result the woman cannot become pregnant and consults a doctor. The fallopian tubes may be partially affected, leading to ectopic pregnancy.
The third stage is characterized by complete blockage of the tubes, their torsion, which makes pregnancy absolutely impossible.
How do adhesions in the pelvis hurt?
Symptoms of adhesions in the pelvis resemble menstrual sensations - abdominal pain, tingling in the appendages, constant aching sensations in the back.
Adhesions of the pelvic organs do not hurt only at the initial stage of development of the pathology.
Therefore, women are not even aware of such a disease, which needs to be treated as quickly as possible.
Adhesions hurt at a later stage, when pathological processes cover large areas.
Symptoms of uterine adhesions can be expressed by irregular menstruation - too short or too long a cycle, and the menstruation itself is extremely painful.
During the intermenstrual period, during adhesions, vaginal discharge with characteristic inflammatory characteristics, an admixture of pus, and an unpleasant odor may occur.
If there are symptoms of pelvic adhesions, treatment should be started as soon as possible - at an early stage of the development of pathology, it is much easier to eliminate the adhesion using conservative methods than to dissect it surgically.
Classification
The clinical classification of doctors of any specialty is based on the characteristics of pelvioperitonitis with the subsequent formation of connective tissue cords.
| Form | Manifestations |
| Acute course | Clinical symptoms are pronounced. Vivid pain and intoxication syndromes, body temperature rises to febrile levels. Signs of peritoneal irritation are positive. There may be intestinal paresis with the development of obstruction. |
| Intermittent flow | The course of the disease consists of periods of exacerbations and remissions. Characterized by low-intensity painful sensations and a slight rise in temperature (not higher than 38 degrees). During the period when the process subsides, there are no clinical symptoms. |
| Chronic course | There are either no symptoms at all or they are mild. Periodically, constipation and mild pain in the lower quadrants of the abdomen appear. This type plays a key role in the development of infertility and miscarriage. |
After some time (from 4 weeks to several years) from the moment the inflammation begins, cords begin to form in the pelvis. It should be noted that adhesions are localized not only in the pelvis, but also in the intra-abdominal cavity, but there are significantly fewer of them.
Gynecologists and reproductive specialists distinguish the following stages of the disease depending on the data obtained during laparoscopy.
| Stage | Characteristic |
| I | Single strands, thin adhesions, weakly disrupt organ function. |
| II | Numerous cords, dense. The surface of the ovaries is covered by less than 50%. |
| III | Many dense adhesions cover above half the surface of the ovaries. |
| IV | The adhesions are dense, lamellar, and completely cover the ovaries. The functions of all affected organs are impaired. Vivid pain syndrome. |
How to identify adhesions
An experienced doctor can determine the adhesive process by manually examining the genital organs.
Adhesions in gynecology can be clearly palpated; the immobility of organs or their limited mobility is of great importance.
The plastic process leads to limitation of movements and palpation of cords, which are defining signs regarding adhesions.
In the future, doctors refer the woman for a number of additional studies, during which a definite diagnosis can be made.
Ultrasound
Ultrasound examination is not indicative. Adhesions in the fallopian tubes can only be suspected when their walls are occluded, and the low power of diagnostic devices makes it impossible to see this.
Since it is not possible to detect adhesions with ultrasound, they resort to hysterosalpingography.
Hysterosalpingography
Fallopian tube adhesions can be seen during hysterosalpingography. In this study, the uterine cavity is filled with a contrast agent, the boundaries of which are determined by ultrasound or x-ray.
The analysis assumes the greatest filling of the organ, during which it is possible to determine the presence of occlusion in the fallopian tubes.
Diagnostics
Diagnosis of pathology begins with collecting the patient’s history and complaints. Conducting a gynecological examination makes it possible to establish limited mobility of the uterus, shortening of the vaginal vaults; upon palpation in the area of the appendages, pain is determined and heaviness is felt. Additional examination includes:
Diagnostic laparoscopy. The method allows you to identify pelvic adhesions in 100% of cases. If necessary, diagnostic laparoscopy is converted into therapeutic laparoscopy - dissection of adhesions.- Ultrasound of the pelvic organs. The reliability of the method reaches 90 – 100%. Adhesions are visualized as irregular echoes that connect the pelvic walls and organs.
- Metrosalpingography. An X-ray examination method allows you to determine the patency of the fallopian tubes.
- MRI of the pelvic organs. The images show anechoic white adhesions.
In order to identify the microbial agent that provoked chronic inflammation, smears are taken for vaginal flora, bacterial culture of vaginal contents and determination of antibiotic sensitivity of detected microorganisms, PCR for latent sexually transmitted infections.
Why are adhesions dangerous?
Adhesive disease of the pelvis is a formidable pathology that can provoke severe complications. First of all, this is infertility, which many women are afraid of.
Also, fusion threatens to disrupt the functioning of internal organs and intestines, which can lead to its obstruction.
Without proper treatment, patients are at risk of adenomyosis. To prevent adhesions from causing complications, the disease must be treated when the first symptoms appear.
Symptoms
A woman experiences pain syndrome - an unpleasant sensation in the suprapubic, lumbosacral region of the back. The intensity of discomfort varies: basically, it is constant, but dull in nature, without localization at a specific point. Factors that provoke increased pain are heavy lifting, psycho-emotional stress, ovulation, menstruation and hypothermia. If film growths in the pelvis are not eliminated for a long time, even defecation and urination are accompanied by severe discomfort.
Other symptoms of the condition:
- Digestive disorders (loud intestinal motility, flatulence, constipation, or vice versa - diarrhea)
- Dyspeptic symptoms (nausea, vomiting)
- Increased body temperature (often develops as a result of psycho-emotional stress caused by pain)
The listed symptoms arise due to compression of the internal organs by overgrown adhesions.
Causes
The adhesive process occurs for several reasons, but the “palm” in this matter should be given to inflammatory processes.
It is in the presence of infections of the appendages, peritoneum and uterus that the risk of occlusions arises most, and streptococci occupy the leading position among representatives of pathogenic microflora.
The supposed causes of adhesions in the fallopian tubes are long-term use of a contraceptive IUD, abortion and diagnostic curettage of the organ, and sexually transmitted diseases.
Pathologies of the digestive system, for example, appendicitis, can provoke the appearance of occlusion.
Adhesions appear in the abdominal cavity and pelvis due to traumatic injuries to organs, rupture of the ovaries, and injuries to the abdominal organs. Adhesions also appear as a result of endometriosis.
Clinical manifestations
At the onset of the disease, pain comes to the fore. The pain is dull, low-intensity and localized mainly in the lower abdomen. Gradually, the severity of the symptom increases - strong, aching, with irradiation to the area of the sacrum, rectum, and upper abdomen.
Any physical activity (running, lifting weights, sexual intercourse) causes increased pain. The location of adhesions in the pelvic area determines the characteristics of the clinical picture. When the peri-rectal tissue and the rectum itself are affected, pain develops during the act of defecation, in the bladder - during the act of urination or excessive filling of the organ with urine, in the area of the ureters - constantly, in the lateral parts of the abdomen.
Damage to the ovaries is dangerous. Pain always occurs during ovulation, stress, and psycho-emotional overload. Infertility develops quickly, since the ovarian tissues cannot fully perform their function. There may be involvement of the fallopian tubes, which “overgrow from the inside” and completely block the path of the egg on its way to the uterine cavity.
With a long course and extensive damage to the peritoneum and pelvic organs, disorders of the gastrointestinal tract are added:
- unstable stool – alternating periods of constipation and diarrhea;
- flatulence, accompanied by a sharp increase in pain;
- periodic nausea and vomiting, with intestinal obstruction - vomiting of intestinal contents.
Prevention
Fallopian tube adhesions are easier to prevent than to treat, so much attention is paid to the prevention of pathology. The basic principles of preventing the formation of synechiae are as follows:
- careful treatment of abdominal tissues - this advice applies, first of all, to doctors performing abdominal interventions;
- taking anti-inflammatory hormonal and non-hormonal drugs that will help calm down inflammatory processes;
- use, if necessary, antifibrotic drugs that promote rapid dissolution of fibrin strands;
- the use of medications aimed at reducing the accumulation of collagen and elastin - the main building components of adhesions;
- prevention of sexually transmitted diseases;
- timely detection and treatment of inflammatory pathologies of the pelvic organs;
- prevention of abortions, individual selection of contraceptive drugs;
- When using spirals, it is important not to miss the deadline for replacing the spiral, and have this done by highly qualified specialists.
If you follow all preventive measures, it is quite possible to avoid adhesions even after complex surgical interventions.